Department of Psychiatry, University of Minnesota Medical School, Minneapolis.
Centre for Emotional Health, Macquarie University, Sydney, Australia.
JAMA Netw Open. 2018 Nov 2;1(7):e185354. doi: 10.1001/jamanetworkopen.2018.5354.
Multivariable comorbidity research indicates that childhood adversity increases the risk for the development of common mental disorders. This risk is explained by underlying internalizing and externalizing transdiagnostic constructs that are amplified by environmental stressors. The differential susceptibility model suggests that this interaction of risk and environment is bidirectional: at-risk individuals will have worse outcomes in high-stress environments but better outcomes in in low-stress environments.
To test the differential susceptibility model by examining how a history of adverse childhood experiences moderates the association between life stress and transdiagnostic psychopathology.
DESIGN, SETTING, AND PARTICIPANTS: Data came from the US National Epidemiological Survey on Alcohol and Related Conditions (NESARC), a population-based observational longitudinal survey administered to adults (≥18 years of age). Participants completed the survey at wave 1 (from 2001 through 2002) and wave 2 (from 2004 through 2005). Responses from 34 458 participants were used for the analyses from March 3, 2017, through October 8, 2018.
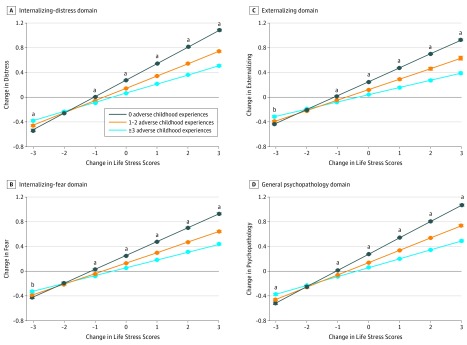
Latent variables for internalizing-fear, internalizing-distress, externalizing, and general psychopathology were created to represent continuous levels of psychopathology in each wave. Latent variables were also created to represent continuous levels of life stress at each wave. Level of childhood adversity was characterized based on the number of types of childhood adversity experienced (no [0 types], low [1-2 types], and high [≥3 types] exposure). Analyses examined how the interaction between level of childhood adversity and adult life stress was associated with change in adult transdiagnostic psychopathology factors.
Of the 34 458 participants included in the analysis (58.0% women and 42.0% men; mean [SD] age, 46.0 [17.4] years at wave 1 and 49.0 [17.3] years at wave 2), 40.5% had no adverse childhood experiences, 34.6% had 1 to 2, and 24.9% had 3 or more. At wave 1, 61.5% of the sample endorsed at least 1 stressful life event and 27.2% met criteria for at least 1 mental disorder; at wave 2, these figures were 64.7% and 29.7%, respectively. Childhood adversity moderated the association between changes in adult life stress and changes in all transdiagnostic psychopathology factors. Specifically, higher levels of childhood adversity had a stronger association between adult life stress and adult transdiagnostic psychopathology factors. Further, significant differences between childhood adversity groups occurred in the mean scores of all transdiagnostic psychopathology factors for both increases and decreases in life stress, providing preliminary evidence of differential susceptibility.
Results provide empirical support for childhood adversity as a differential susceptibility factor engendering heightened functional and dysfunctional reactivity to later stress.
多变量合并症研究表明,童年逆境会增加常见精神障碍的发展风险。这种风险可以通过潜在的内化和外化的跨诊断结构来解释,这些结构会被环境压力放大。差异易感性模型表明,这种风险与环境的相互作用是双向的:处于风险中的个体在高压力环境中的结果会更差,但在低压力环境中的结果会更好。
通过研究童年期不良经历史如何调节生活压力与跨诊断精神病理学之间的关系,来检验差异易感性模型。
设计、地点和参与者:数据来自美国全国酒精相关情况流行病学调查(NESARC),这是一项基于人群的观察性纵向调查,对象为成年人(≥18 岁)。参与者在第 1 波(2001 年至 2002 年)和第 2 波(2004 年至 2005 年)完成了调查。从 2017 年 3 月 3 日至 2018 年 10 月 8 日,对来自 34458 名参与者的回复进行了分析。
为了代表每一波的连续心理病理学水平,创建了内化-恐惧、内化-痛苦、外化和一般精神病理学的潜在变量。还创建了代表每一波生活压力的连续水平的潜在变量。童年逆境的水平是根据经历的童年逆境类型的数量来描述的(0 种[0 类型]、1-2 种[1-2 类型]和≥3 种[≥3 类型]暴露)。分析考察了童年逆境水平与成年生活压力之间的相互作用与成年跨诊断精神病理学因素变化之间的关系。
在纳入分析的 34458 名参与者中(58.0%为女性,42.0%为男性;第 1 波平均[SD]年龄为 46.0[17.4]岁,第 2 波为 49.0[17.3]岁),40.5%的参与者没有不良的童年经历,34.6%的参与者有 1 到 2 种,24.9%的参与者有 3 种或更多。在第 1 波,61.5%的样本至少有 1 个压力生活事件,27.2%符合至少 1 种精神障碍的标准;在第 2 波,这一数字分别为 64.7%和 29.7%。童年逆境调节了成年生活压力变化与所有跨诊断精神病理学因素变化之间的关系。具体来说,童年逆境程度越高,成年生活压力与成年跨诊断精神病理学因素之间的关联就越强。此外,在生活压力增加和减少时,所有跨诊断精神病理学因素的平均得分在童年逆境群体之间存在显著差异,为差异易感性提供了初步证据。
结果为童年逆境作为差异易感性因素提供了实证支持,这种因素导致对后期压力的功能和非功能反应增强。