Patient Safety, Global Medicines Development, AstraZeneca, Pepparedsleden 1, Mölndal, 431 83, Sweden.
Global Medicines Development, AstraZeneca, Granta Park, Great Abington, Cambridge, CB21 6GH, UK.
Drug Saf. 2019 Jun;42(6):769-784. doi: 10.1007/s40264-018-00788-w.
Tralokinumab is a monoclonal antibody (mAb) that neutralizes interleukin (IL)-13, a cytokine involved in the pathogenesis of asthma.
The objectives of this study were to characterize the potential immunogenic properties of tralokinumab and report data for anti-drug antibodies (ADAs) and hypersensitivity reactions from two phase III clinical trials.
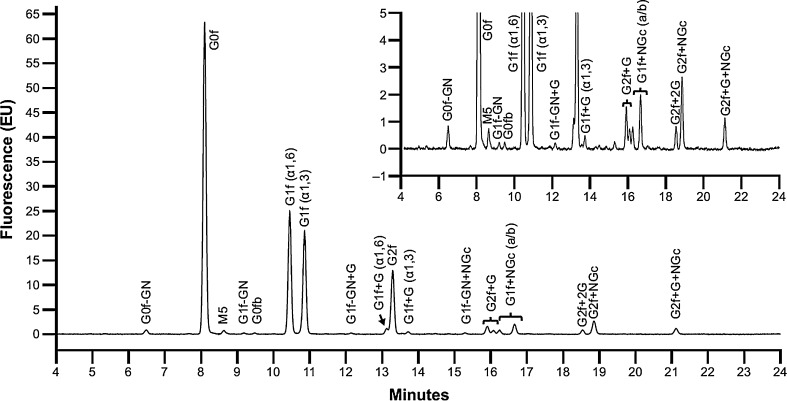
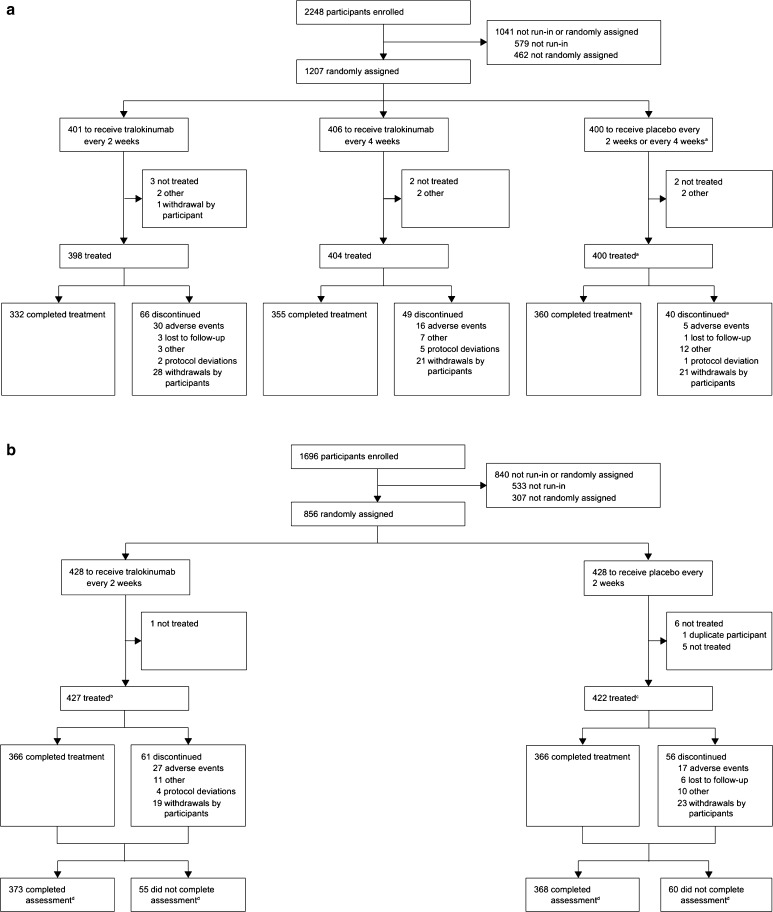
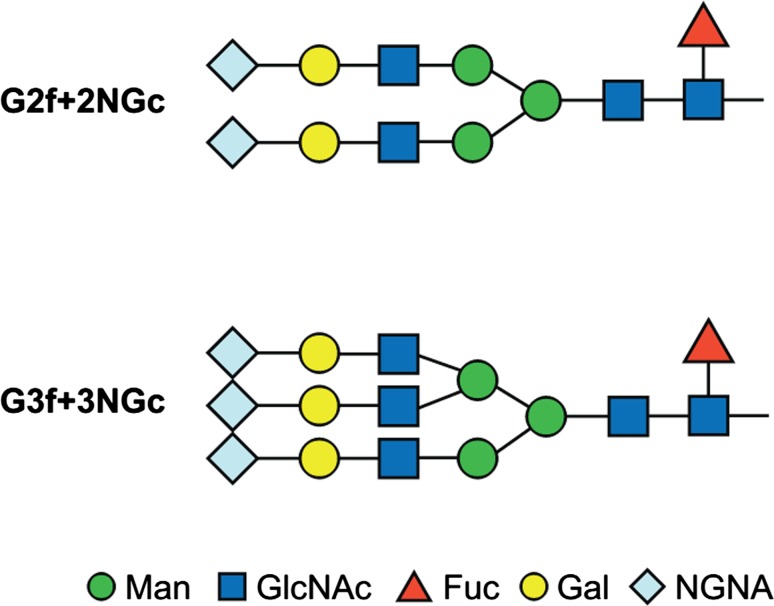
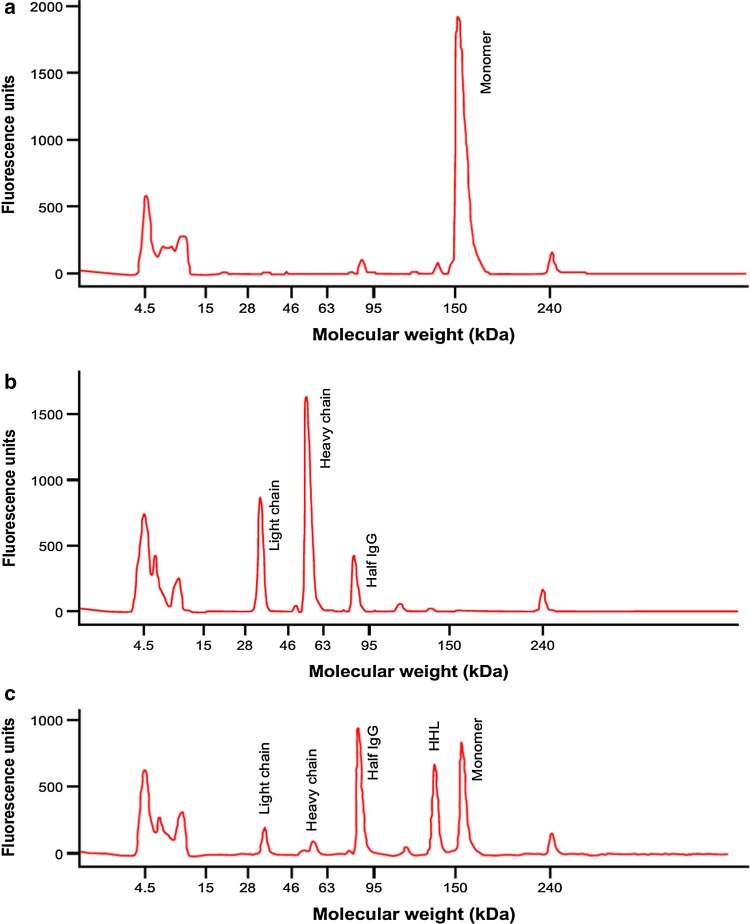
The oligosaccharide structure of tralokinumab, Fab-arm exchange, and ADAs were characterized by standard techniques. Hypersensitivity adverse events (AEs) were evaluated in two pivotal clinical trials of tralokinumab in severe, uncontrolled asthma: STRATOS 1 and 2 (NCT02161757 and NCT02194699).
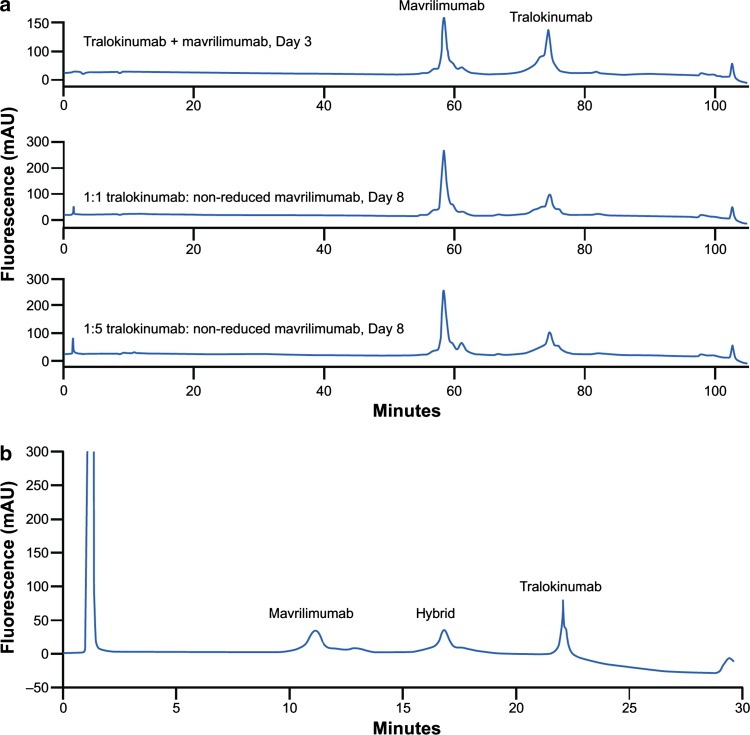
No galactose-α-1,3-galactose (α-Gal) epitopes were found in the Fab region of tralokinumab and only 4.5% of glycoforms contained α-Gal in the Fc region. Under non-reducing conditions, Fab-arm exchange did not take place with another immunoglobulin (Ig) G mAb (mavrilimumab). However, following glutathione reduction, a hybrid antibody with monovalent bioactivity was detected. ADA incidences (titers) were as follows: STRATOS 1-every 2 weeks (Q2 W) 0.8% (26.0), every 4 weeks (Q4 W) 0.5% (26.0), placebo 0.8% (52.0); STRATOS 2-Q2 W 1.2% (39.0), placebo 0.8% (13.0). Participant-reported hypersensitivity AE rates were as follows: STRATOS 1-Q2 W 25.9%, Q4 W 25.0%, placebo 25.5%; STRATOS 2-Q2 W 13.2%, placebo 9.0%. External evaluation for anaphylaxis by Sampson criteria found no tralokinumab-related severe hypersensitivity or anaphylaxis reactions.
Preclinical assessments suggested a low likelihood of immunogenicity for tralokinumab. In STRATOS 1 and 2, ADA incidence was low, no differences were found between tralokinumab-treated and placebo groups in reporting of hypersensitivity reactions, and there were no Sampson criteria-evaluated anaphylaxis events with tralokinumab treatment. Together, the results suggest that tralokinumab treatment would not increase the risk for severe hypersensitivity or anaphylactic reactions.
特利鲁单抗是一种单克隆抗体(mAb),可中和白细胞介素(IL)-13,这种细胞因子参与哮喘的发病机制。
本研究的目的是描述特利鲁单抗的潜在免疫原性特征,并报告两项 III 期临床试验中抗药物抗体(ADA)和过敏反应的数据。
采用标准技术对特利鲁单抗的寡糖结构、Fab 臂交换和 ADA 进行了表征。在两项特利鲁单抗治疗严重、未控制的哮喘的关键临床试验 STRATOS 1 和 2(NCT02161757 和 NCT02194699)中评估了过敏反应不良事件(AE)。
特利鲁单抗 Fab 区域未发现半乳糖-α-1,3-半乳糖(α-Gal)表位,仅 4.5%的糖型在 Fc 区域含有 α-Gal。在非还原条件下,Fab 臂交换不会与另一种免疫球蛋白(Ig)G mAb(马伏鲁单抗)发生。然而,在谷胱甘肽还原后,检测到具有单价生物活性的杂交抗体。ADA 发生率(滴度)如下:STRATOS 1-每 2 周(Q2W)0.8%(26.0),每 4 周(Q4W)0.5%(26.0),安慰剂 0.8%(52.0);STRATOS 2-Q2W 1.2%(39.0),安慰剂 0.8%(13.0)。报告的过敏反应 AE 发生率如下:STRATOS 1-Q2W 25.9%,Q4W 25.0%,安慰剂 25.5%;STRATOS 2-Q2W 13.2%,安慰剂 9.0%。Sampson 标准的过敏反应外部评估未发现与特利鲁单抗相关的严重过敏或过敏反应。
临床前评估表明特利鲁单抗的免疫原性较低。在 STRATOS 1 和 2 中,ADA 发生率较低,特利鲁单抗治疗组与安慰剂组报告的过敏反应无差异,且特利鲁单抗治疗无 Sampson 标准评估的过敏反应事件。综上所述,特利鲁单抗治疗不会增加严重过敏或过敏反应的风险。