Child Health Research Center, Division of Respiratory Medicine, Allergy, and Immunology, Department of Pediatrics, University of Virginia School of Medicine, Charlottesville, Va.
Division of Allergy, Asthma, and Immunology, Department of Medicine, University of Virginia School of Medicine, Charlottesville, Va.
J Allergy Clin Immunol Pract. 2019 Jul-Aug;7(6):1803-1812.e10. doi: 10.1016/j.jaip.2018.12.027. Epub 2019 Jan 14.
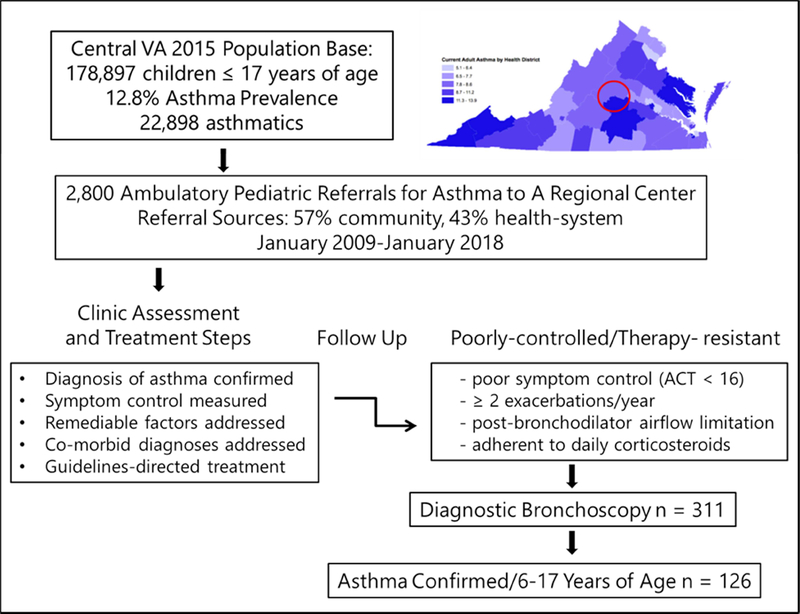
Children with severe asthma have frequent exacerbations despite guidelines-based treatment with high-dose corticosteroids. The importance of refractory lung inflammation and infectious species as factors contributing to poorly controlled asthma in children is poorly understood.
To identify prevalent granulocyte patterns and potential pathogens as targets for revised treatment, 126 children with severe asthma underwent clinically indicated bronchoscopy.
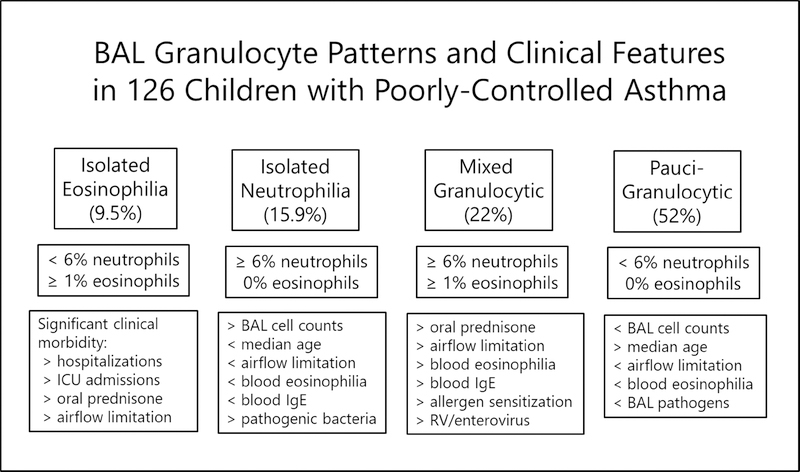
Diagnostic tests included bronchoalveolar lavage (BAL) for cell count and differential, bacterial and viral studies, spirometry, and measurements of blood eosinophils, total IgE, and allergen-specific IgE. Outcomes were compared among 4 BAL granulocyte patterns.
Pauci-granulocytic BAL was the most prevalent granulocyte category (52%), and children with pauci-granulocytic BAL had less postbronchodilator airflow limitation, less blood eosinophilia, and less detection of BAL enterovirus compared with children with mixed granulocytic BAL. Children with isolated neutrophilia BAL were differentiated by less blood eosinophilia than those with mixed granulocytic BAL, but greater prevalence of potential bacterial pathogens compared with those with pauci-granulocytic BAL. Children with isolated eosinophilia BAL had features similar to those with mixed granulocytic BAL. Children with mixed granulocytic BAL took more maintenance prednisone, and had greater blood eosinophilia and allergen sensitization compared with those with pauci-granulocytic BAL.
In children with severe, therapy-resistant asthma, BAL granulocyte patterns and infectious species are associated with novel phenotypic features that can inform pathway-specific revisions in treatment. In 32% of children evaluated, BAL revealed corticosteroid-refractory eosinophilic infiltration amenable to anti-T2 biological therapies, and in 12%, a treatable bacterial pathogen.
尽管根据指南使用大剂量皮质类固醇治疗,但患有严重哮喘的儿童仍会频繁发作。导致儿童哮喘控制不佳的难治性肺部炎症和感染性病原体的重要性尚未得到充分理解。
为了确定常见的粒细胞模式和潜在的病原体作为修订治疗的靶点,126 名患有严重哮喘的儿童接受了临床指征下的支气管镜检查。
诊断测试包括支气管肺泡灌洗(BAL)细胞计数和分类、细菌和病毒研究、肺活量测定以及血液嗜酸性粒细胞、总 IgE 和过敏原特异性 IgE 的测量。比较了 4 种 BAL 粒细胞模式的结果。
少粒细胞性 BAL 是最常见的粒细胞类别(52%),与混合粒细胞性 BAL 相比,少粒细胞性 BAL 的儿童支气管扩张后气流受限程度较低,血液嗜酸性粒细胞计数较低,BAL 肠道病毒检测率较低。与混合粒细胞性 BAL 相比,单纯性中性粒细胞性 BAL 的儿童血液嗜酸性粒细胞计数较低,但与少粒细胞性 BAL 相比,潜在细菌病原体的流行率更高。单纯性嗜酸性粒细胞性 BAL 的儿童具有与混合粒细胞性 BAL 相似的特征。与少粒细胞性 BAL 相比,混合粒细胞性 BAL 的儿童服用更多的维持性泼尼松,且血液嗜酸性粒细胞计数和过敏原致敏率更高。
在患有严重、治疗抵抗性哮喘的儿童中,BAL 粒细胞模式和感染性病原体与新的表型特征相关,这些特征可告知特定途径的治疗修订。在评估的 32%的儿童中,BAL 显示出对 T2 生物疗法有反应的皮质类固醇难治性嗜酸性粒细胞浸润,在 12%的儿童中发现了可治疗的细菌病原体。