Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, England.
Sheffield Hallam University, Montgomery House, 32 Collegiate Crescent, Sheffield, S10 2BP, England.
BMC Geriatr. 2019 Jan 18;19(1):15. doi: 10.1186/s12877-019-1031-4.
Polypharmacy, and the associated adverse drug events such as non-adherence to prescriptions, is a common problem for elderly people living with multiple comorbidities. Deprescribing, i.e. the gradual withdrawal from medications with supervision by a healthcare professional, is regarded as a means of reducing adverse effects of multiple medications including non-adherence. This systematic review examines the evidence of deprescribing as an effective strategy for improving medication adherence amongst older, community dwelling adults.
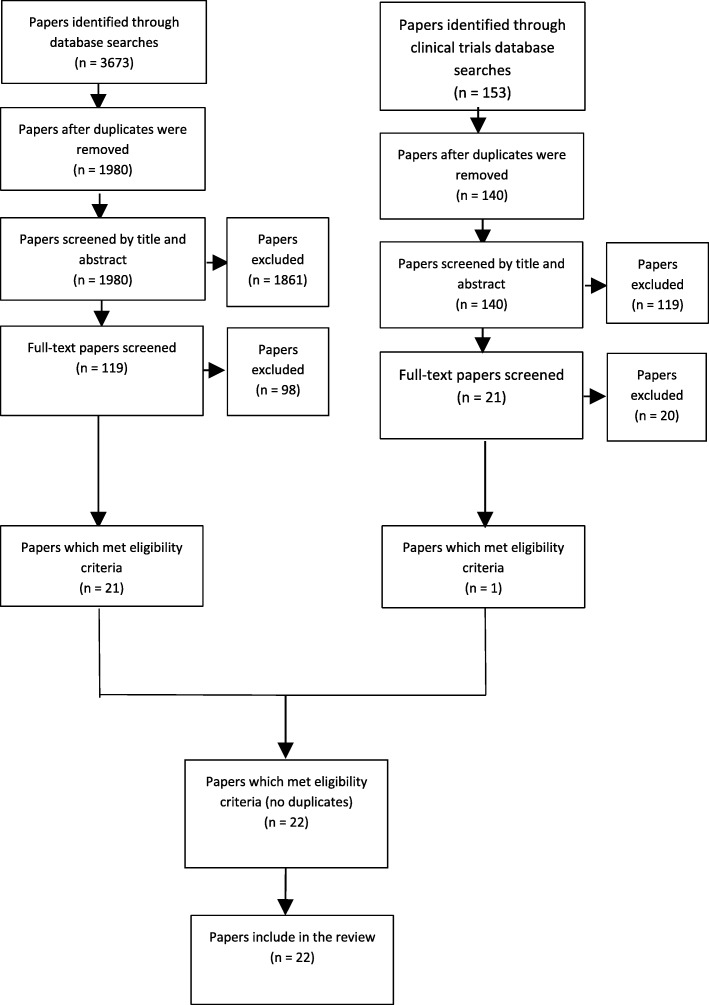
A mixed methods review was undertaken. Eight bibliographic database and two clinical trials registers were searched between May and December 2017. Results were double screened in accordance with pre-defined inclusion/exclusion criteria related to polypharmacy, deprescribing and adherence in older, community dwelling populations. The Mixed Methods Appraisal Tool (MMAT) was used for quality appraisal and an a priori data collection instrument was used. For the quantitative studies, a narrative synthesis approach was taken. The qualitative data was analysed using framework analysis. Findings were integrated using a mixed methods technique. The review was performed in accordance with the PRISMA reporting statement.
A total of 22 original studies were included, of which 12 were RCTs. Deprescribing with adherence as an outcome measure was identified in randomised controlled trials (RCTs), observational and cohort studies from 13 countries between 1996 and 2017. There were 17 pharmacy-led interventions; others were led by General Practitioners (GP) and nurses. Four studies demonstrated an overall reduction in medications of which all studies corresponded with improved adherence. A total of thirteen studies reported improved adherence of which 5 were RCTs. Adherence was reported as a secondary outcome in all but one study.
There is insufficient evidence to show that deprescribing improves medication adherence. Only 13 studies (of 22) reported adherence of which only 5 were randomised controlled trials. Older people are particularly susceptible to non-adherence due to multi-morbidity associated with polypharmacy. Bio-psycho-social factors including health literacy and multi-disciplinary team interventions influence adherence. The authors recommend further study into the efficacy and outcomes of medicines management interventions. A consensus on priority outcome measurements for prescribed medications is indicated.
PROSPERO number CRD42017075315.
老年人同时患有多种疾病,因此会同时服用多种药物,这导致药物滥用和药物不良反应(如不遵医嘱)的情况十分常见。减少药物副作用(包括不遵医嘱)的一种方法是逐渐减少药物剂量,即撤药。本系统综述考察了撤药作为一种提高社区居住的老年患者药物依从性的有效策略的证据。
采用混合方法综述。2017 年 5 月至 12 月,检索了 8 个文献数据库和 2 个临床试验注册处。根据与老年人、社区居住人群中的药物滥用、撤药和依从性相关的预先设定的纳入/排除标准,对结果进行了双重筛选。采用混合方法评估工具(MMAT)对质量进行评估,并使用预先确定的数据收集工具。对于定量研究,采用叙述性综合方法。使用框架分析对定性数据进行分析。使用混合方法技术整合研究结果。本综述符合 PRISMA 报告声明。
共纳入 22 项原始研究,其中 12 项为 RCT。在 1996 年至 2017 年间,从 13 个国家的随机对照试验(RCT)、观察性研究和队列研究中确定了以依从性为结局指标的撤药。这些研究涉及 17 项药房主导的干预措施;其他干预措施由全科医生和护士主导。四项研究表明药物总体减少,所有研究均对应依从性提高。共有 13 项研究报告了依从性提高,其中 5 项为 RCT。除一项研究外,其余研究均将依从性作为次要结局进行报告。
目前尚无充分证据表明撤药可以提高药物依从性。仅有 13 项研究(共 22 项)报告了依从性,其中仅有 5 项为 RCT。老年人由于与药物滥用相关的多种疾病而特别容易出现不遵医嘱的情况。生物-心理-社会因素(包括健康素养和多学科团队干预)会影响依从性。作者建议进一步研究药物管理干预措施的疗效和结果。还需要就优先考虑的处方药物疗效测量达成共识。
PROSPERO 编号 CRD42017075315。