HRB Centre for Primary Care Research, Department of General Practice, Royal College of Surgeons in Ireland, University of Medicine and Health Sciences, Dublin, Ireland.
Data Science Centre, Royal College of Surgeons in Ireland, University of Medicine and Health Sciences, Dublin, Ireland.
PLoS Med. 2022 Jan 5;19(1):e1003862. doi: 10.1371/journal.pmed.1003862. eCollection 2022 Jan.
There is a rising prevalence of multimorbidity, particularly in older patients, and a need for evidence-based medicines management interventions for this population. The Supporting Prescribing in Older Adults with Multimorbidity in Irish Primary Care (SPPiRE) trial aimed to investigate the effect of a general practitioner (GP)-delivered, individualised medication review in reducing polypharmacy and potentially inappropriate prescriptions (PIPs) in community-dwelling older patients with multimorbidity in primary care.
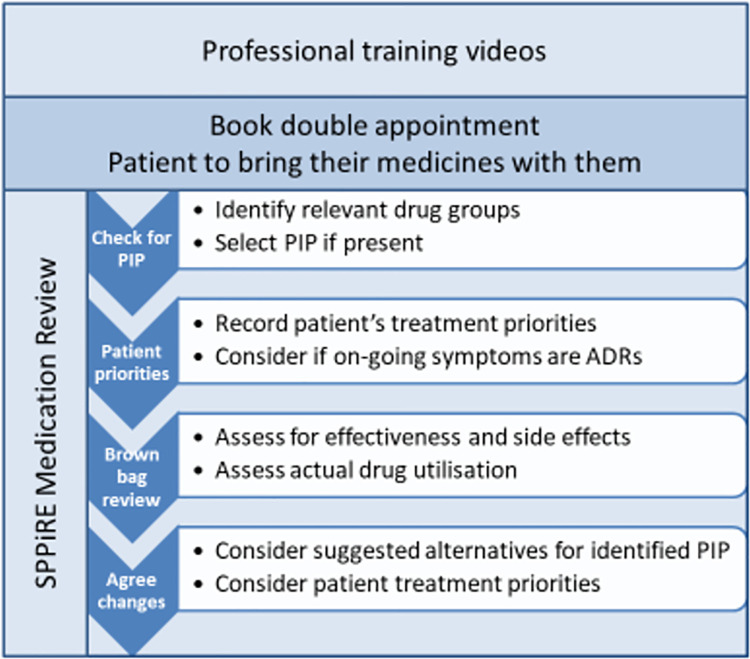
We conducted a cluster randomised controlled trial (RCT) set in 51 GP practices throughout the Republic of Ireland. A total of 404 patients, aged ≥65 years with complex multimorbidity, defined as being prescribed ≥15 regular medicines, were recruited from April 2017 and followed up until October 2020. Furthermore, 26 intervention GP practices received access to the SPPiRE website where they completed an educational module and used a template for an individualised patient medication review that identified PIP, opportunities for deprescribing, and patient priorities for care. A total of 25 control GP practices delivered usual care. An independent blinded pharmacist assessed primary outcome measures that were the number of medicines and the proportion of patients with any PIP (from a predefined list of 34 indicators based predominantly on the STOPP/START version 2 criteria). We performed an intention-to-treat analysis using multilevel modelling. Recruited participants had substantial disease and treatment burden at baseline with a mean of 17.37 (standard deviation [SD] 3.50) medicines. At 6-month follow-up, both intervention and control groups had reductions in the numbers of medicines with a small but significantly greater reduction in the intervention group (incidence rate ratio [IRR] 0.95, 95% confidence interval [CI]: 0.899 to 0.999, p = 0.045). There was no significant effect on the odds of having at least 1 PIP in the intervention versus control group (odds ratio [OR] 0.39, 95% CI: 0.140 to 1.064, p = 0.066). Adverse events recorded included mortality, emergency department (ED) presentations, and adverse drug withdrawal events (ADWEs), and there was no evidence of harm. Less than 2% of drug withdrawals in the intervention group led to a reported ADWE. Due to the inability to electronically extract data, primary outcomes were measured at just 2 time points, and this is the main limitation of this work.
The SPPiRE intervention resulted in a small but significant reduction in the number of medicines but no evidence of a clear effect on PIP. This reduction in significant polypharmacy may have more of an impact at a population rather than individual patient level.
ISRCTN Registry ISRCTN12752680.
随着人口老龄化的加剧,多重疾病的发病率不断上升,尤其是在老年患者中,因此需要针对这一人群提供基于证据的药物管理干预措施。在爱尔兰初级医疗保健中支持老年多重疾病患者处方的研究(SPPiRE)旨在调查由全科医生(GP)实施的个体化药物审查对减少社区居住的多重疾病老年患者的药物滥用和潜在不适当处方(PIP)的影响。
我们进行了一项集群随机对照试验(RCT),该试验在爱尔兰共和国的 51 家全科医生诊所进行。共有 404 名年龄≥65 岁、患有复杂多重疾病的患者(定义为服用≥15 种常规药物),他们于 2017 年 4 月至 2020 年 10 月被招募,并进行了随访。此外,26 家干预性全科医生诊所可以访问 SPPiRE 网站,在该网站上,他们完成了一个教育模块,并使用了一个用于个体化患者药物审查的模板,以确定 PIP、去处方机会和患者护理重点。25 家对照性全科医生诊所提供常规护理。一位独立的盲审药剂师评估了主要结局指标,即药物数量和任何 PIP(根据基于 STOPP/START 版本 2 标准的 34 个指标的预定义清单确定)的患者比例。我们使用多层次建模进行了意向治疗分析。招募的参与者在基线时就有大量的疾病和治疗负担,平均服用 17.37 种(标准差 [SD] 3.50)药物。在 6 个月的随访中,干预组和对照组的药物数量都有所减少,干预组的减少幅度较小,但具有统计学意义(发生率比 [IRR] 0.95,95%置信区间 [CI]:0.899 至 0.999,p = 0.045)。干预组与对照组相比,至少有 1 个 PIP 的可能性没有显著影响(比值比 [OR] 0.39,95%CI:0.140 至 1.064,p = 0.066)。记录的不良事件包括死亡率、急诊科(ED)就诊和药物不良停药事件(ADWE),但没有证据表明存在危害。干预组中不到 2%的药物停药导致报告了 ADWE。由于无法电子提取数据,主要结局指标仅在 2 个时间点进行了测量,这是该研究的主要局限性。
SPPiRE 干预措施导致药物数量略有但显著减少,但没有证据表明 PIP 有明显影响。这种显著的药物滥用减少可能在人群层面而非个体患者层面产生更大的影响。
ISRCTN 注册 ISRCTN8041300。