Medical University of South Carolina, Department of Surgery, Charleston, SC, USA.
Northwell Health, Manhasset, NY, USA.
Clin Pharmacol Drug Dev. 2019 Nov;8(8):995-1008. doi: 10.1002/cpdd.657. Epub 2019 Jan 22.
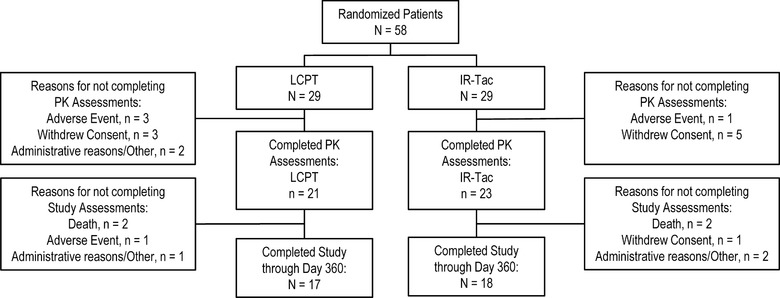
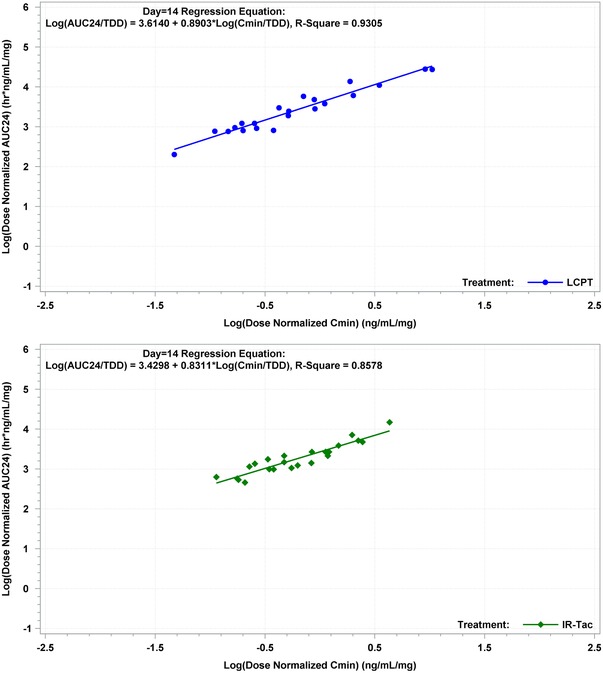
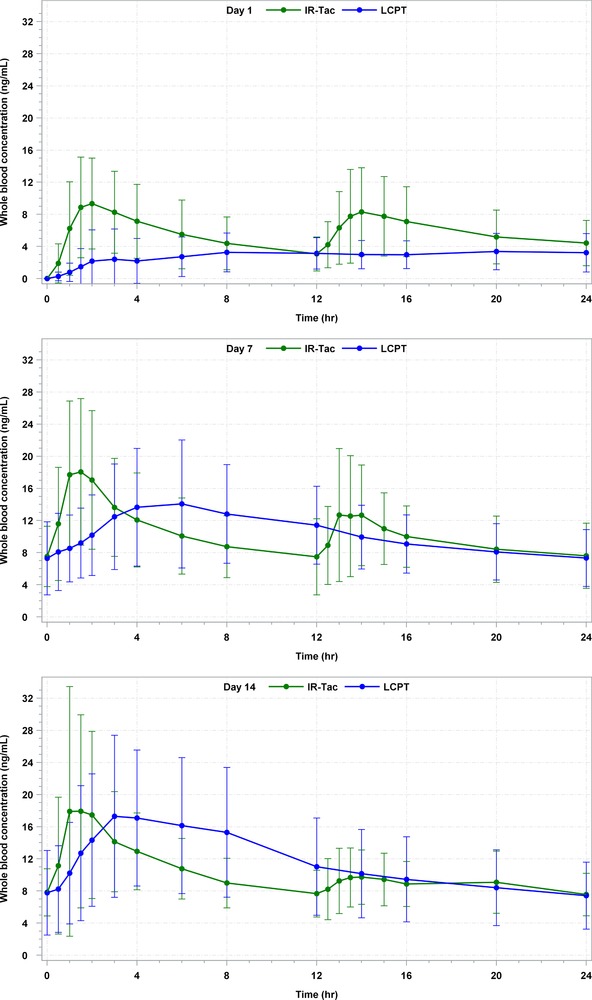
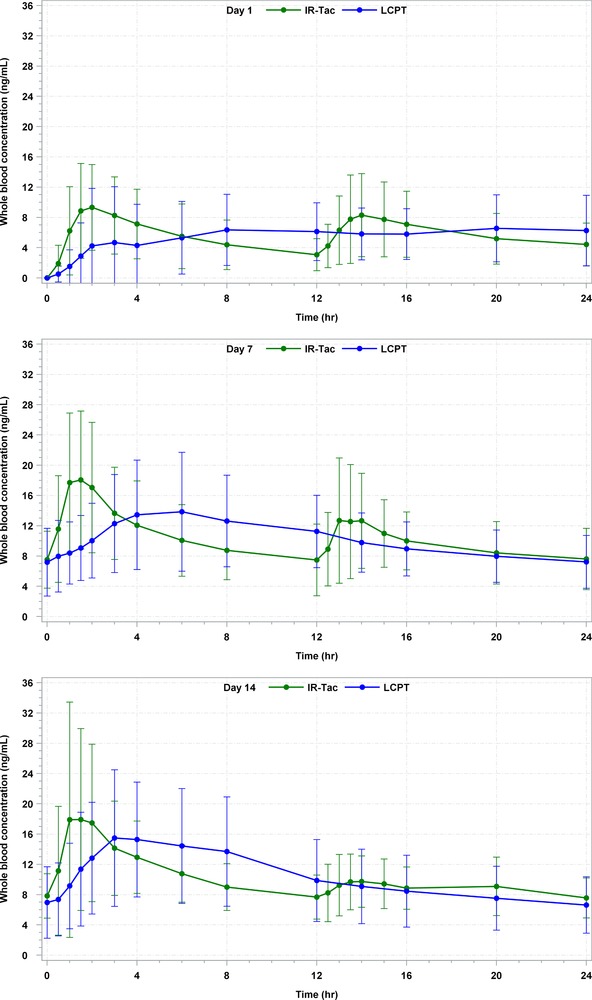
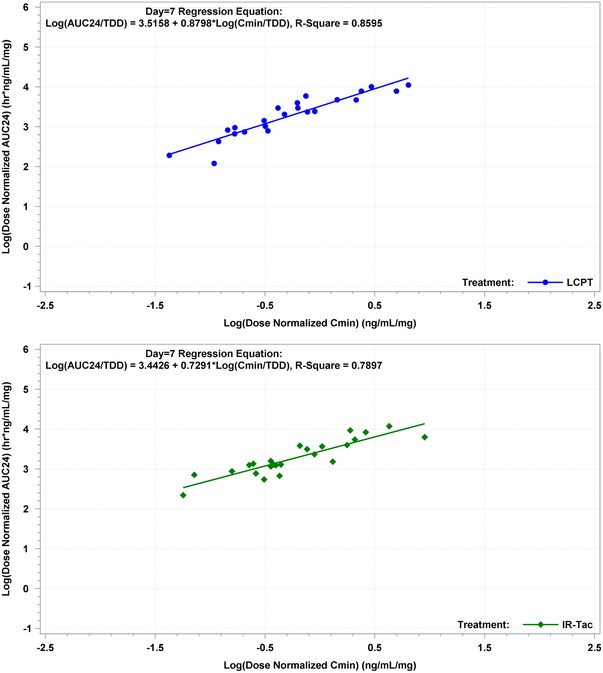
The pharmacokinetics of once-daily extended-release tacrolimus tablets (LCPT) in de novo liver transplantation have not been previously reported. In this phase II, randomized, open-label study, de novo liver transplant recipients were randomized to LCPT 0.07-0.13 mg/kg/day (taken once daily; n = 29) or twice-daily immediate-release tacrolimus capsules (IR-Tac) at 0.10-0.15 mg/kg/day (divided twice daily; n = 29). Subsequent doses of both drugs were adjusted to maintain tacrolimus trough concentrations of 5 to 20 ng/mL through day 90, and 5-15 ng/mL thereafter. Twenty-four-hour pharmacokinetic profiles were obtained on days 1, 7, and 14, with trough concentration and efficacy/safety monitoring through year 1. Similar proportions of patients in both groups achieved therapeutic trough concentrations on days 7 and 14 (day 7: LCPT = 78%, IR-Tac = 75%; day 14: LCPT = 86%, IR-Tac = 91%) as well as similar systemic and peak exposure. There was a robust correlation between drug concentration at time 0 and area under the concentration-time curve for both LCPT and IR-Tac (respectively, day 7: r = 0.86 and 0.79; day 14: r = 0.93 and 0.86; P < .0001 for all). Dose adjustments during days 1 to 14 were frequent. Thirty-five patients completed the extended-use period. No significant differences in adverse events were seen between groups. Incidence of biopsy-proven acute rejection (LCPT = 6 and IR-Tac = 4) was similar on day 360. Between formulations, overall exposure was similar at 1 week after transplant with the characteristic delayed-release pharmacokinetic profile of LCPT demonstrated in this novel population. These data support further investigation of the safety and efficacy of LCPT in de novo liver transplantation.
在肝移植中,每日一次的延长释放他克莫司片(LCPT)的药代动力学尚未被报道过。在这项 II 期、随机、开放标签研究中,将新诊断的肝移植受者随机分为 LCPT 0.07-0.13mg/kg/天(每日一次;n=29)或每日两次的即时释放他克莫司胶囊(IR-Tac)0.10-0.15mg/kg/天(分两次服用;n=29)。两种药物的后续剂量均进行调整,以在第 90 天内维持他克莫司谷浓度为 5 至 20ng/mL,并在此后维持 5-15ng/mL。在第 1、7 和 14 天获得 24 小时药代动力学曲线,并在第 1 年内进行谷浓度和疗效/安全性监测。两组患者在第 7 天和第 14 天均有相似比例的患者达到治疗性谷浓度(第 7 天:LCPT=78%,IR-Tac=75%;第 14 天:LCPT=86%,IR-Tac=91%),且全身暴露和峰值暴露相似。LCPT 和 IR-Tac 的药物浓度与时间 0 的相关性均很强(分别为第 7 天:r=0.86 和 0.79;第 14 天:r=0.93 和 0.86;P<0.0001)。第 1 天至第 14 天期间频繁调整剂量。35 例患者完成了延长使用期。两组之间的不良事件发生率无显著差异。第 360 天的活检证实的急性排斥反应发生率(LCPT=6 例,IR-Tac=4 例)相似。两种制剂之间,在移植后 1 周时的总体暴露相似,LCPT 具有其独特的延迟释放药代动力学特征,在该新型人群中得到了证实。这些数据支持进一步研究 LCPT 在新诊断肝移植中的安全性和疗效。