1 Nephrology Department of Clinical and Experimental Medicine University of Catania Italy.
2 Department of Gastroenterology Gulhane School of Medicine Etlik, Ankara Turkey.
J Am Heart Assoc. 2019 Feb 5;8(3):e010942. doi: 10.1161/JAHA.118.010942.
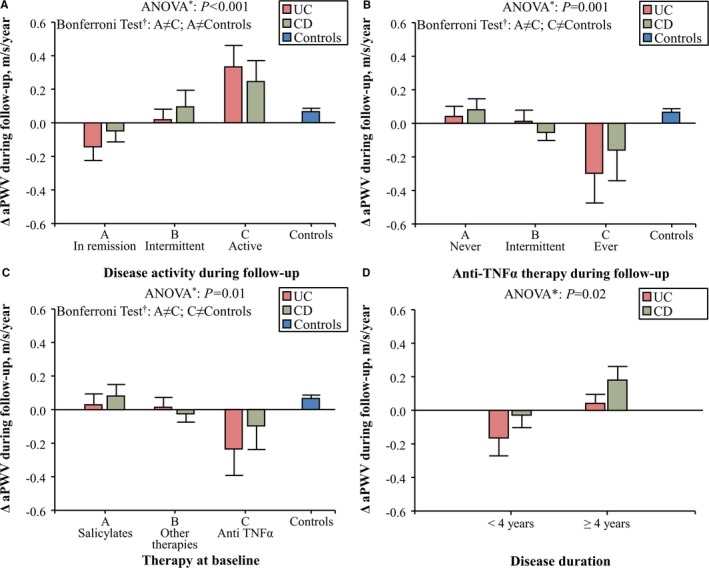
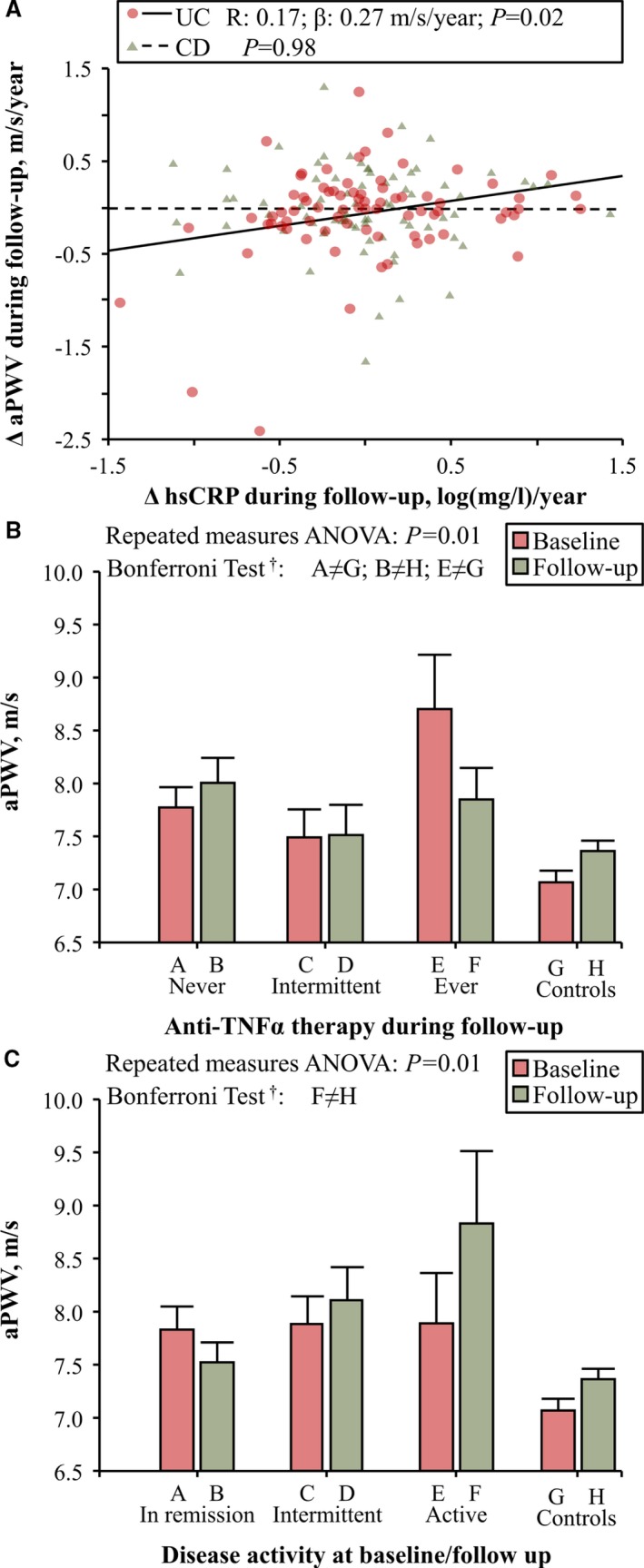
Background Inflammatory bowel disease ( IBD ) is characterized by a low prevalence of traditional risk factors, an increased aortic pulse-wave velocity ( aPWV ), and an excess of cardiovascular events. We have previously hypothesized that the cardiovascular risk excess reported in these patients could be explained by chronic inflammation. Here, we tested the hypothesis that chronic inflammation is responsible for the increased aPWV previously reported in IBD patients and that anti-TNFa (anti-tumor necrosis factor-alpha) therapy reduce aPWV in these patients. Methods and Results This was a multicenter longitudinal study. We enrolled 334 patients: 82 patients with ulcerative colitis, 85 patients with Crohn disease, and 167 healthy control subjects matched for age, sex, and mean blood pressure, from 3 centers in Europe, and followed them for 4 years (range, 2.5-5.7 years). At baseline, IBD patients had higher aPWV than controls. IBD patients in remission and those treated with anti-TNFa during follow-up experienced an aortic destiffening, whereas aPWV increased in those with active disease and those treated with salicylates ( P=0.01). Disease duration ( P=0.02) was associated with aortic stiffening as was, in patients with ulcerative colitis, high-sensitivity C-reactive protein during follow-up ( P=0.02). All these results were confirmed after adjustment for major confounders. Finally, the duration of anti-TNFa therapy was not associated with the magnitude of the reduction in aPWV at the end of follow-up ( P=0.85). Conclusions Long-term anti-TNFa therapy reduces aPWV , an established surrogate measure of cardiovascular risk, in patients with IBD . This suggests that effective control of inflammation may reduce cardiovascular risk in these patients.
炎症性肠病(IBD)的特点是传统危险因素的患病率较低、主动脉脉搏波速度(aPWV)增加以及心血管事件增多。我们之前假设,这些患者报告的心血管风险增加可能是由慢性炎症引起的。在这里,我们检验了这样一个假设,即慢性炎症是导致先前报道的 IBD 患者 aPWV 增加的原因,并且抗 TNFa(抗肿瘤坏死因子-α)治疗可以降低这些患者的 aPWV。
这是一项多中心纵向研究。我们纳入了来自欧洲 3 个中心的 334 名患者:82 名溃疡性结肠炎患者、85 名克罗恩病患者和 167 名年龄、性别和平均血压匹配的健康对照者,随访时间为 4 年(范围 2.5-5.7 年)。基线时,IBD 患者的 aPWV 高于对照组。缓解期 IBD 患者和随访期间接受抗 TNFa 治疗的患者经历了主动脉僵硬度降低,而活动期疾病患者和接受柳氮磺胺吡啶治疗的患者 aPWV 增加(P=0.01)。疾病持续时间(P=0.02)与主动脉僵硬度相关,在溃疡性结肠炎患者中,随访期间的高敏 C 反应蛋白也与主动脉僵硬度相关(P=0.02)。所有这些结果在调整了主要混杂因素后仍然成立。最后,抗 TNFa 治疗的持续时间与随访结束时 aPWV 降低的幅度无关(P=0.85)。
长期抗 TNFa 治疗可降低 IBD 患者的 aPWV,aPWV 是心血管风险的一个既定替代指标。这表明有效控制炎症可能会降低这些患者的心血管风险。