Komeyama Shotaro, Takagi Kensuke, Tsuboi Hideyuki, Tsuboi Shigeki, Morita Yasuhiro, Yoshida Ruka, Kanzaki Yasunori, Nagai Hiroaki, Ikai Yoshihiro, Furui Koichi, Tsuzuki Kazuhito, Shibata Naoki, Yoshioka Naoki, Yamauchi Ryota, Sugiyama Hiroki, Morishima Itsuro
Department of Cardiology, Ogaki Municipal Hospital, Japan.
Department of Emergency, Ogaki Municipal Hospital, Japan.
Intern Med. 2019 May 15;58(10):1391-1397. doi: 10.2169/internalmedicine.0864-18. Epub 2019 Feb 1.
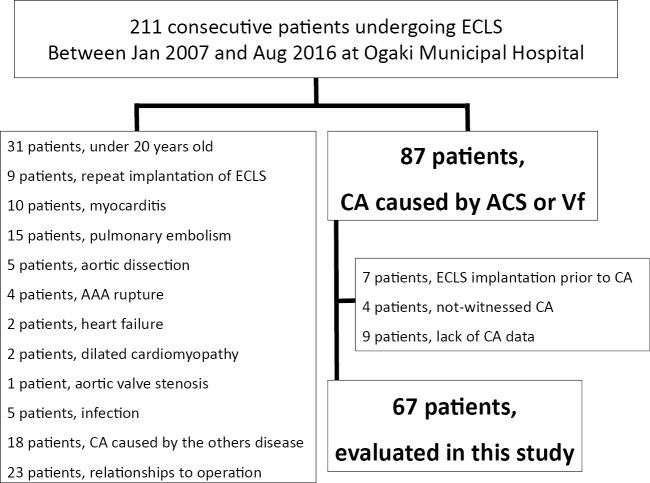
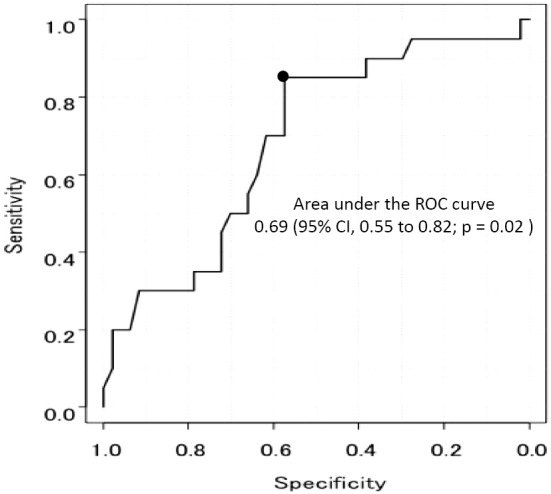
Objective Extracorporeal life support (ECLS) is effective for improving the survival rate of patients with refractory cardiac arrest (rCA). As little data are available regarding the impact of ECLS on a favorable neurological outcome, the predictors of a favorable neurological outcome were evaluated in this study. Methods Between January 2007 and August 2016, we retrospectively recruited patients with rCA caused by cardiac events treated with ECLS in our institute. A favorable neurological outcome was defined as a Glasgow-Pittsburgh cerebral performance category score 1 at discharge. The study endpoint was the clinical outcomes and predictors of favorable neurologic patients at discharge. Results During the study period, 67 patients with CA caused by cardiac events (acute coronary syndrome, 57 patients; idiopathic ventricular fibrillation, 10 patients) were included. Of these, 20 patients (29.9%) were classified into the favorable neurological group. No marked difference was observed in the patient characteristics between those with and without a favorable outcome except for in the time from CA to starting ECLS (ECLS initiation time). A short ECLS initiation time resulted in a favorable outcome (37.8±28.1 minutes vs. 53.6±30.7 minutes, p=0.05). The cut-off time of ECLS initiation was 46 minutes, which was prolonged by the temporary return of spontaneous circulation before ECLS [odds ratio (OR), 3.69; 95% confidence interval (CI), 1.34-10.19; p=0.01] and transfer to the angiographic room (OR, 4.07; 95% CI, 1.44-11.53, p=0.008). Conclusion The early initiation of ECLS (within 46 minutes) might be associated with a favorable neurological outcome for patients with rCA caused by cardiac events.
目的 体外生命支持(ECLS)对提高难治性心脏骤停(rCA)患者的生存率有效。由于关于ECLS对良好神经功能转归影响的数据较少,本研究对良好神经功能转归的预测因素进行了评估。方法 2007年1月至2016年8月,我们回顾性纳入了在我院接受ECLS治疗的由心脏事件导致的rCA患者。良好神经功能转归定义为出院时格拉斯哥-匹兹堡脑功能分类评分1分。研究终点为出院时良好神经功能患者的临床结局及预测因素。结果 在研究期间,纳入了67例由心脏事件导致心脏骤停的患者(急性冠状动脉综合征57例;特发性室颤10例)。其中,20例患者(29.9%)被分类为良好神经功能组。除了从心脏骤停至开始ECLS的时间(ECLS启动时间)外,有良好转归和无良好转归患者的特征未观察到明显差异。较短的ECLS启动时间导致良好转归(37.8±28.1分钟 vs. 53.6±30.7分钟,p=0.05)。ECLS启动的截断时间为46分钟,这在ECLS前因自主循环短暂恢复而延长[比值比(OR),3.69;95%置信区间(CI),1.34-10.19;p=0.01]以及转至血管造影室时延长(OR,4.07;95%CI,1.44-11.53,p=0.008)。结论 对于由心脏事件导致rCA的患者,早期启动ECLS(46分钟内)可能与良好神经功能转归相关。