School of Public Health, University of Queensland, Brisbane, Australia.
School of Population and Global Health, University of Melbourne, Parkville, Australia.
BMC Med. 2019 Feb 8;17(1):29. doi: 10.1186/s12916-019-1267-z.
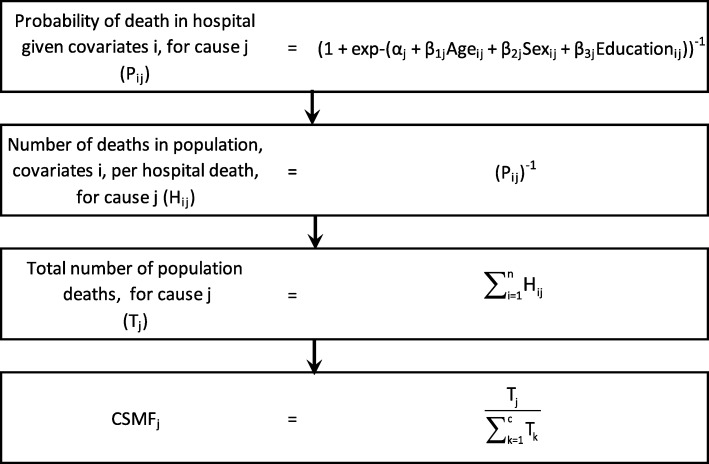
Almost all countries without complete vital registration systems have data on deaths collected by hospitals. However, these data have not been widely used to estimate cause of death (COD) patterns in populations because only a non-representative fraction of people in these countries die in health facilities. Methods that can exploit hospital mortality statistics to reliably estimate community COD patterns are required to strengthen the evidence base for disease and injury control programs. We propose a method that weights hospital-certified causes by the probability of death to estimate population cause-specific mortality fractions (CSMFs).
We used an established verbal autopsy instrument (VAI) to collect data from hospital catchment areas in Chandpur and Comilla Districts, Bangladesh, and Bohol province, the Philippines, between 2011 and 2014, along with demographic covariates for each death. Hospital medical certificates of cause of death (death certificates) were collected and mapped to the corresponding cause categories of the VAI. Tariff 2.0 was used to assign a COD for community deaths. Logistic regression models were created for broad causes in each country to calculate the probability of in-hospital death, given a set of covariate values. The reweighted CSMFs for deaths in the hospital catchment population, represented by each hospital death, were calculated from the corresponding regression models.
We collected data on 4228 adult deaths in the Philippines and 3725 deaths in Bangladesh. Short time to hospital and education were consistently associated with in-hospital death in the Philippines and absence of a disability was consistently associated with in-hospital death in Bangladesh. Non-communicable diseases (excluding stroke) and stroke were the leading causes of death in both the Philippines (33.9%, 19.1%) and Bangladesh (46.1%, 21.1%) according to the reweighted method. The reweighted method generally estimated CSMFs that fell between those derived from hospitals and those diagnosed by Tariff 2.0.
Statistical methods can be used to derive estimates of cause-specific probability of death in-hospital for Bangladesh and the Philippines to generate population CSMFs. In regions where hospital death certification is of reasonable quality and routine verbal autopsy is not applied, these estimates could be applied to generate cost-effective and robust CSMFs for the population.
几乎所有没有完整生命登记系统的国家都有医院收集的死亡数据。然而,由于这些国家只有一小部分人在卫生机构死亡,这些数据尚未被广泛用于估计人群的死因(COD)模式。需要能够利用医院死亡率统计数据可靠估计社区 COD 模式的方法,以加强疾病和伤害控制计划的证据基础。我们提出了一种通过死亡概率对医院认证死因进行加权的方法,以估计人群特定死因的死亡率分数(CSMF)。
我们使用一种已建立的口述尸检工具(VAI),于 2011 年至 2014 年期间在孟加拉国的钱德普尔和科米拉区以及菲律宾的保和省的医院集水区收集数据,以及每个死亡病例的人口统计学协变量。收集了医院死亡证明(死亡证明)并将其映射到 VAI 的相应死因类别。Tariff 2.0 用于为社区死亡分配 COD。为每个国家的广泛死因创建了逻辑回归模型,以计算给定一组协变量值时在医院死亡的概率。根据相应的回归模型,从每个医院死亡代表的医院集水区人群死亡中计算出加权后的 CSMF。
我们在菲律宾收集了 4228 例成人死亡数据,在孟加拉国收集了 3725 例死亡数据。在菲律宾,到医院的时间短和教育程度高与住院死亡始终相关,而在孟加拉国,没有残疾与住院死亡始终相关。非传染性疾病(不包括中风)和中风是菲律宾(分别为 33.9%和 19.1%)和孟加拉国(分别为 46.1%和 21.1%)的主要死因。根据加权方法,非传染性疾病(不包括中风)和中风是菲律宾(分别为 33.9%和 19.1%)和孟加拉国(分别为 46.1%和 21.1%)的主要死因。加权方法通常估计的 CSMF 介于由医院得出的 CSMF 和 Tariff 2.0 诊断得出的 CSMF 之间。
可以使用统计方法来为孟加拉国和菲律宾推导医院内特定死因的死亡概率估计值,以生成人群 CSMF。在医院死亡证明质量合理且常规口述尸检未应用的地区,这些估计值可用于为人群生成具有成本效益且稳健的 CSMF。