Department of Rheumatology, Gaetano Pini Institute, Milan, Italy.
Pfizer Innovative Health, I&I Medical Affairs, Rome, Italy.
Biomed Res Int. 2019 Jan 10;2019:6107217. doi: 10.1155/2019/6107217. eCollection 2019.
To retrospectively evaluate the impact of comorbidities on treatment choice, 12-month clinical response, and 24-month retention rate in a cohort of patients with rheumatoid arthritis (RA) treated with a first-line tumor necrosis factor alpha inhibitor (TNFi), by using for the first time the Rheumatic Disease Comorbidity Index (RDCI).
The study population was extracted from a local registry of RA patients receiving adalimumab or etanercept as first-line biologics between January 2001 and December 2013. The prevalence of comorbidities was computed, and patients were stratified according to RDCI for evaluating the role of comorbidities on TNFi choice, concomitant methotrexate, clinical response (1-year DAS28-ESR remission and low disease activity [LDA] and EULAR good-moderate response), and the 24-month retention rate.
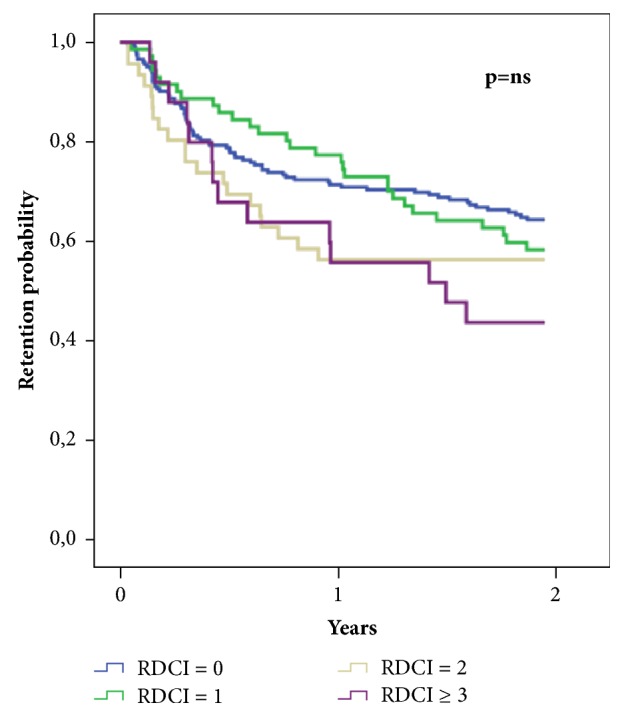
346 patients (172 adalimumab and 174 etanercept) were included. A significantly higher EULAR good/moderate response ( 0.020) and DAS28-ESR remission ( 0.003) were obtained according to RDCI (0, 1, 2, or ≥3). Lower RDCI ( 0.022), male sex ( 0.006), higher baseline DAS28-ESR ( 0.001), ETN ( < 0.001), and concomitant methotrexate ( 0.016) were predictors of EULAR good/moderate response. Elevated RDCI was a predictor of discontinuation of biologics ( 0.036), whereas treatment with etanercept ( < 0.001) and methotrexate ( 0.007) was associated with a lower risk of TNFi withdrawal.
Multimorbidity, measured by RDCI, is a negative predictor of TNFi persistence on treatment and of achieving a good clinical response. The use of RDCI may be very useful for identifying patients with RA carrying those comorbid conditions associated with poor prognostic outcomes and for defining new treatment targets in multimorbid RA patients.
本研究旨在首次使用风湿病合并症指数(RDCI),回顾性评估合并症对接受一线肿瘤坏死因子-α抑制剂(TNFi)治疗的类风湿关节炎(RA)患者的治疗选择、12 个月临床缓解和 24 个月保留率的影响。
从 2001 年 1 月至 2013 年 12 月接受阿达木单抗或依那西普作为一线生物制剂的 RA 患者的本地登记处提取研究人群。计算合并症的患病率,并根据 RDCI 评估合并症对 TNFi 选择、伴随甲氨蝶呤、临床缓解(1 年 DAS28-ESR 缓解和低疾病活动[LDA]和 EULAR 良好/中等反应)和 24 个月保留率的作用。
共纳入 346 例患者(阿达木单抗 172 例,依那西普 174 例)。根据 RDCI(0、1、2 或≥3),RDCI 评分越高,EULAR 良好/中等反应(0.020)和 DAS28-ESR 缓解(0.003)的获得率越高。RDCI 评分较低(0.022)、男性(0.006)、基线 DAS28-ESR 较高(0.001)、ETN(<0.001)和伴随甲氨蝶呤(0.016)是 EULAR 良好/中等反应的预测因子。升高的 RDCI 是生物制剂停药的预测因子(0.036),而依那西普(<0.001)和甲氨蝶呤(0.007)的治疗与 TNFi 停药的风险降低相关。
RDCI 衡量的合并症是 TNFi 治疗持续存在和实现良好临床反应的负面预测因子。RDCI 的使用可能非常有助于识别合并那些与预后不良相关的合并症的 RA 患者,并为合并症 RA 患者确定新的治疗靶点。