Kariyama Kazuya, Nouso Kazuhiro, Toyoda Hidenori, Tada Toshifumi, Hiraoka Atsushi, Tsuji Kunihiko, Itobayashi Ei, Ishikawa Toru, Wakuta Akiko, Oonishi Ayano, Kumada Takashi, Kudo Masatoshi, Group On Behalf Of The Real-Life Practice Experts For Hcc Relpec Study, Group Hcc
Department of Gastroenterology and Liver Disease Center, Okayama City Hospital, Okayama 700-8557, Japan.
Department of Gastroenterology and Hepatology, Ogaki Municipal Hospital, Gifu 503-0864, Japan.
Cancers (Basel). 2019 Feb 10;11(2):203. doi: 10.3390/cancers11020203.
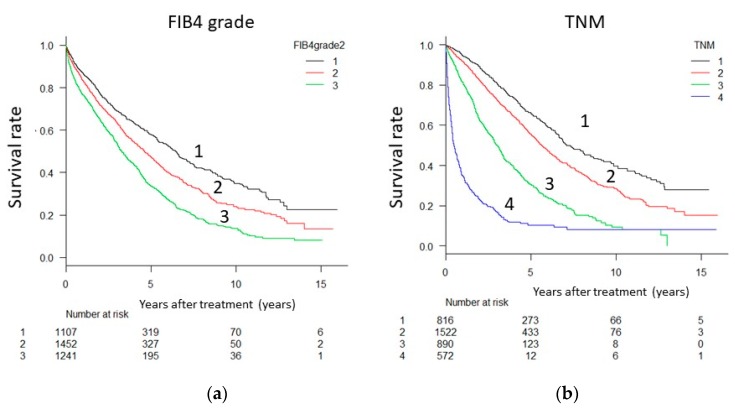
Most integrated scores for predicting the prognosis of patients with hepatocellular carcinoma (HCC) comprise tumor progression factors and liver function variables. The FIB4 index is an indicator of hepatic fibrosis calculated on the basis of age, aspartate aminotransferase (AST) levels, alanine aminotransferase (ALT) levels, and platelet count, but it does not include variables directly related to liver function. We propose a new staging system, referred to as "FIB4-T," comprising the FIB4 index as well as tumor progression factors, and examine its usefulness.
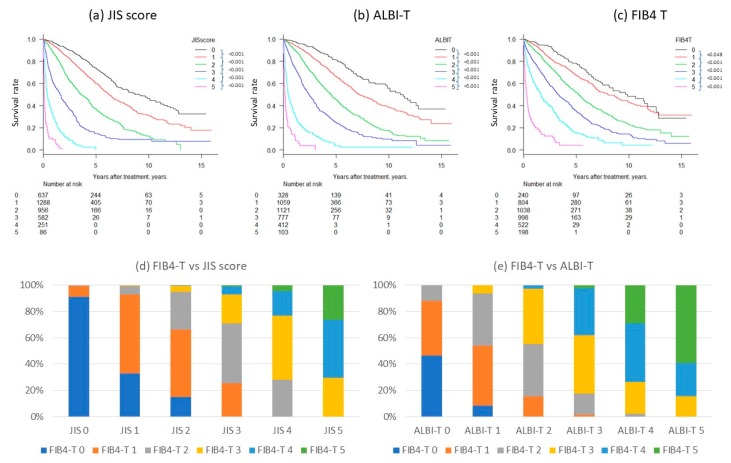
Subjects included 3800 cases of HCC registered in multiple research centers. We defined grades 1, 2, and 3 as a Fibrosis-4 (FIB4) index of <3.25, 3.26⁻6.70, and >6.70 as FIB4, respectively, and calculated the FIB4-T in the same manner in which the JIS (Japan Integrated Staging Score) scores and albumin-bilirubin tumor node metastasis (ALBI-T) were calculated. We compared the prognostic prediction ability of FIB4-T with that of the JIS score and ALBI-T.
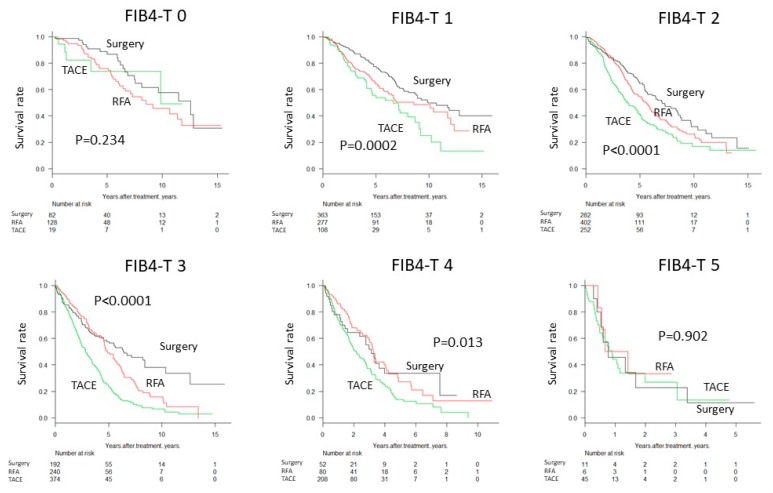
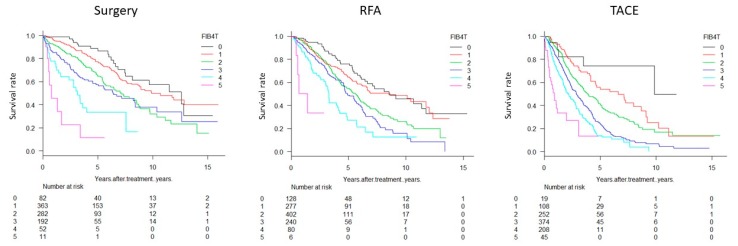
Mean observation period was 37 months. The 5-year survival rates (%) of JIS score (0/1/2/3/4/5), ALBI-T (0/1/2/3/4/5) and FIB4-T (0/1/2/3/4/5) were 74/60/36/16/0, 82/66/45/22/5/0 and 88/75/65/58/32/10, respectively. Comparisons of the Akaike information criteria among JIS scores, ALBI-T, and FIB4-T indicated that stratification using the FIB4-T system was comparable to those using ALBI-T and JIS score. The risk of mortality significantly increased (1.3⁻2.8 times/step) with an increase in FIB4-T, and clear stratification was possible regardless of the treatment.
FIB4-T is useful in predicting the prognosis of patients with HCC from a new perspective.
大多数用于预测肝细胞癌(HCC)患者预后的综合评分包括肿瘤进展因素和肝功能变量。FIB4指数是一种基于年龄、天冬氨酸转氨酶(AST)水平、丙氨酸转氨酶(ALT)水平和血小板计数计算得出的肝纤维化指标,但它不包括与肝功能直接相关的变量。我们提出了一种新的分期系统,称为“FIB4-T”,它包括FIB4指数以及肿瘤进展因素,并检验其有效性。
研究对象包括在多个研究中心登记的3800例HCC病例。我们将1级、2级和3级分别定义为Fibrosis-4(FIB4)指数<3.25、3.26⁻6.70和>6.70,并且以计算日本综合分期评分(JIS)和白蛋白-胆红素肿瘤淋巴结转移分期(ALBI-T)的相同方式计算FIB4-T。我们比较了FIB4-T与JIS评分和ALBI-T对预后的预测能力。
平均观察期为37个月。JIS评分(0/1/2/3/4/5)、ALBI-T(0/1/2/3/4/5)和FIB4-T(0/1/2/3/4/5)的5年生存率(%)分别为74/60/36/16/0、82/66/45/22/5/0和88/75/65/58/32/10。JIS评分、ALBI-T和FIB4-T之间的赤池信息准则比较表明,使用FIB4-T系统进行分层与使用ALBI-T和JIS评分进行分层相当。随着FIB4-T升高,死亡风险显著增加(1.3⁻2.8倍/级),无论治疗方式如何都可以进行明确分层。
FIB4-T从一个新的角度对预测HCC患者的预后是有用的。