Swedish Medical Center/Providence St. Joseph Health and the University of Washington, Seattle, Washington.
University of Toronto, Toronto, Ontario, Canada.
Arthritis Rheumatol. 2019 Jul;71(7):1112-1124. doi: 10.1002/art.40851. Epub 2019 May 28.
To examine the efficacy of methotrexate monotherapy relative to etanercept monotherapy and the value of combining methotrexate and etanercept for the treatment of patients with psoriatic arthritis (PsA).
In this double-blind study, 851 patients with PsA were randomized to 1 of 3 treatment arms, as follows: oral methotrexate (20 mg) plus subcutaneous placebo given weekly (n = 284), subcutaneous etanercept (50 mg) plus oral placebo given weekly (n = 284), or subcutaneous etanercept (50 mg) plus oral methotrexate (20 mg) given weekly (combination therapy; n = 283). The American College of Rheumatology 20% improvement (ACR20) response and Minimal Disease Activity (MDA) response at week 24 were the primary end point and key secondary end point, respectively. Other measures of inflammatory arthritis, radiographic progression, and nonarticular disease manifestations were also assessed.
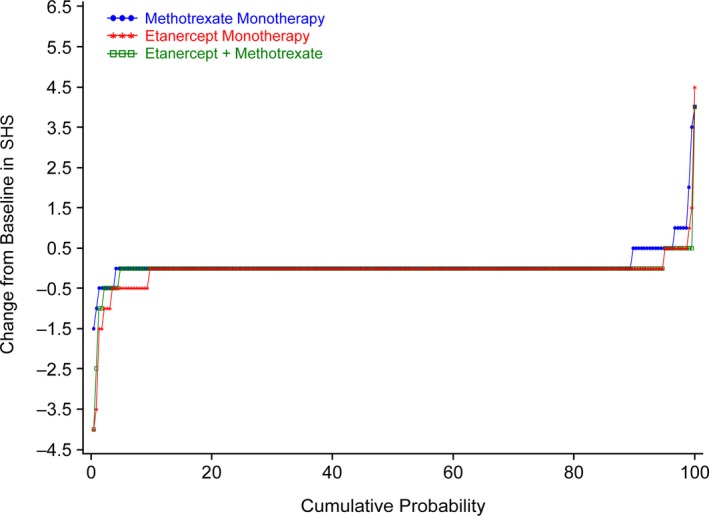
Patients with PsA had a mean ± SD age of 48.4 ± 13.1 years, and the mean ± SD duration of PsA was 3.2 ± 6.3 years (median 0.6 years). ACR20 and MDA response rates at week 24 were significantly greater in patients who received etanercept monotherapy compared with those who received methotrexate monotherapy (ACR20, 60.9% versus 50.7% of patients [P = 0.029]; MDA, 35.9% versus 22.9% of patients [P = 0.005]), and both were significantly greater in the combination therapy group compared with the methotrexate monotherapy group at week 24 (ACR20, 65.0% versus 50.7% of patients [P = 0.005]; MDA, 35.7% versus 22.9% of patients [P = 0.005]). Other secondary outcomes (ACR50 and ACR70 response rates, proportions of patients achieving a Very Low Disease Activity score, and PsA disease activity scores) showed between-group differences that were consistent with the primary and key secondary end point results. Furthermore, patients in both etanercept treatment arms showed less radiographic progression at week 48 compared with patients who received methotrexate monotherapy. Outcomes were similar in the combination therapy and etanercept monotherapy groups, except for some skin end points. No new safety signals were seen.
Etanercept monotherapy and combination therapy with etanercept and methotrexate showed greater efficacy than methotrexate monotherapy in patients with PsA, according to the ACR and MDA response rates and extent of radiographic progression at follow-up. Overall, combining methotrexate and etanercept did not improve the efficacy of etanercept.
研究甲氨蝶呤单药治疗与依那西普单药治疗相比,以及联合甲氨蝶呤和依那西普治疗对银屑病关节炎(PsA)患者的疗效。
在这项双盲研究中,851 例 PsA 患者被随机分配至 3 个治疗组之一,具体如下:每周接受口服甲氨蝶呤(20mg)联合皮下安慰剂治疗(n=284)、每周接受皮下依那西普(50mg)联合口服安慰剂治疗(n=284)或每周接受皮下依那西普(50mg)联合口服甲氨蝶呤(20mg)治疗(联合治疗组;n=283)。第 24 周时美国风湿病学会 20%改善(ACR20)应答和最小疾病活动度(MDA)应答是主要终点和关键次要终点。还评估了其他炎症性关节炎、放射学进展和非关节疾病表现的指标。
PsA 患者的平均年龄±标准差为 48.4±13.1 岁,PsA 的平均病程±标准差为 3.2±6.3 年(中位数 0.6 年)。与接受甲氨蝶呤单药治疗的患者相比,接受依那西普单药治疗的患者在第 24 周时 ACR20 和 MDA 应答率显著更高(ACR20:60.9%与 50.7%的患者[P=0.029];MDA:35.9%与 22.9%的患者[P=0.005]),而联合治疗组与甲氨蝶呤单药治疗组相比,这两个指标在第 24 周时均显著更高(ACR20:65.0%与 50.7%的患者[P=0.005];MDA:35.7%与 22.9%的患者[P=0.005])。其他次要结局(ACR50 和 ACR70 应答率、达到非常低疾病活动度评分的患者比例和 PsA 疾病活动评分)显示出与主要和关键次要终点结果一致的组间差异。此外,与接受甲氨蝶呤单药治疗的患者相比,接受依那西普治疗的两组患者在第 48 周时的放射学进展程度均较低。联合治疗组和依那西普单药治疗组的结局相似,除了一些皮肤终点外。未观察到新的安全性信号。
依那西普单药治疗和依那西普联合甲氨蝶呤治疗在 PsA 患者中的疗效均优于甲氨蝶呤单药治疗,依据是 ACR 和 MDA 应答率以及随访时的放射学进展程度。总体而言,联合应用甲氨蝶呤和依那西普并未提高依那西普的疗效。