Nuffield Department of Orthopaedics, Rheumatology, and Musculoskeletal Sciences, University of Oxford, Oxford, UK.
Department of Dermatology and Department of Medicine, Division of Rheumatology, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
Rheumatology (Oxford). 2021 Mar 2;60(3):1137-1147. doi: 10.1093/rheumatology/keaa271.
To examine which composite measures are most sensitive to change when measuring psoriatic arthritis (PsA) disease activity, analyses compared the responsiveness of composite measures used in a 48-week randomized, controlled trial of MTX and etanercept in patients with PsA.
The trial randomised 851 patients to receive weekly: MTX (20 mg/week), etanercept (50 mg/week) or MTX plus etanercept. Dichotomous composite measures examined included ACR 20/50/70 responses, minimal disease activity (MDA) and very low disease activity (VLDA). Continuous composite measures examined included Disease Activity Score (28 joints) using CRP (DAS28-CRP), Clinical Disease Activity Index (CDAI), Simplified Disease Activity Index (SDAI), Disease Activity for Psoriatic Arthritis (DAPSA) and Psoriatic Arthritis Disease Activity Score (PASDAS).
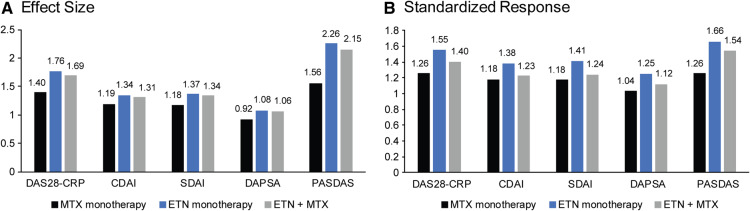
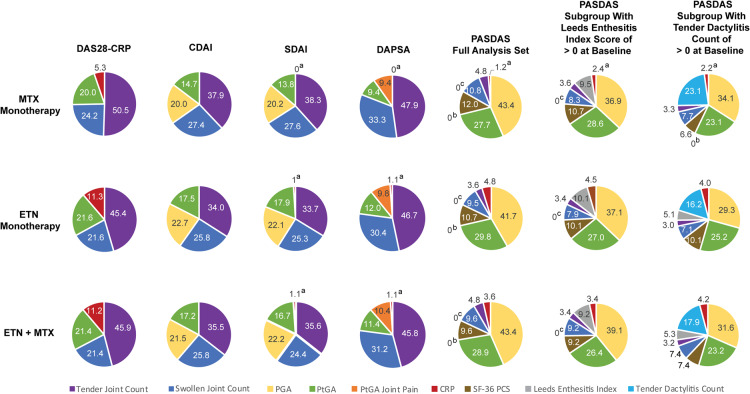
At week 24, etanercept-treated groups were significantly more effective than MTX monotherapy to achieve ACR 20 (primary end point) and MDA (key secondary end point). When examining score changes from baseline at week 24 across the five continuous composite measures, PASDAS demonstrated relatively greater changes in the etanercept-treated groups compared with MTX monotherapy and had the largest effect size and standardized response. Joint count changes drove overall score changes at week 24 from baseline in all the continuous composite measures except for PASDAS, which was driven by the Physician and Patient Global Assessments.
PASDAS was the most sensitive continuous composite measure examined with results that mirrored the protocol-defined primary and key secondary outcomes. Composite measures with multiple domains, such as PASDAS, may better quantify change in PsA disease burden.
https://ClinicalTrials.gov, number NCT02376790.
探讨在评估银屑病关节炎(PsA)疾病活动度时,哪些综合指标的变化最敏感,分析比较了在一项为期 48 周、评估甲氨蝶呤和依那西普治疗 PsA 患者的随机对照试验中使用的综合指标的反应性。
该试验将 851 例患者随机分为每周接受以下治疗的三组:甲氨蝶呤(20mg/周)、依那西普(50mg/周)或甲氨蝶呤联合依那西普。所检查的二分类综合指标包括 ACR20/50/70 反应、最小疾病活动度(MDA)和极低疾病活动度(VLDA)。所检查的连续综合指标包括使用 CRP 的疾病活动评分(28 个关节)(DAS28-CRP)、临床疾病活动指数(CDAI)、简化疾病活动指数(SDAI)、银屑病关节炎疾病活动度评分(DAPSA)和银屑病关节炎疾病活动度评分(PASDAS)。
在第 24 周,依那西普治疗组在实现 ACR20(主要终点)和 MDA(关键次要终点)方面明显比甲氨蝶呤单药治疗更有效。在检查五个连续综合指标中从基线到第 24 周的评分变化时,与甲氨蝶呤单药治疗相比,PASDAS 在依那西普治疗组中显示出相对更大的变化,且具有最大的效应量和标准化反应。除 PASDAS 外,所有连续综合指标的关节计数变化都驱动了第 24 周从基线开始的总体评分变化,PASDAS 则由医生和患者整体评估驱动。
PASDAS 是检查中最敏感的连续综合指标,其结果与方案定义的主要和关键次要结局一致。具有多个领域的综合指标,如 PASDAS,可能更好地量化 PsA 疾病负担的变化。
https://ClinicalTrials.gov,编号 NCT02376790。