Zou Yunlong, Li Ye, Liu Jingchen, Zhang Boyin, Gu Rui
Orthopaedics Surgery Department, China-Japan Union Hospital of Jilin University, Changchun, Jilin Province, China.
Medicine (Baltimore). 2019 Feb;98(7):e14415. doi: 10.1097/MD.0000000000014415.
Gout occurs mainly in joints, but rarely in the spine. In the spine, urate crystals can cause intervertebral space instability but rarely lead to retrolisthesis. Here, we present an extremely rare disease with gout invaded the intervertebral disc with lumbar retrolisthesis.
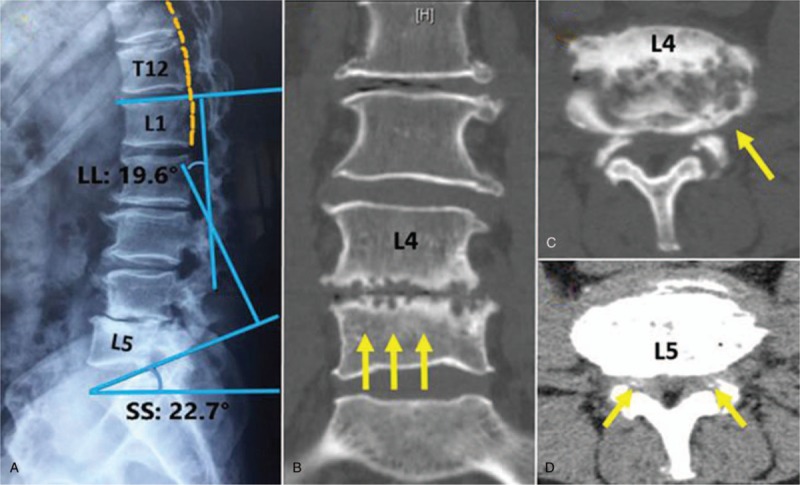
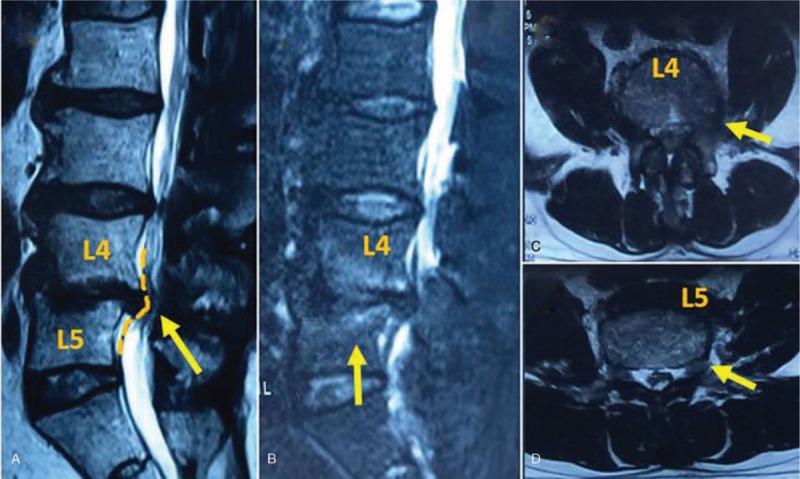
A 61-years male patient with gout history has suffered from severe low back pain and intermittent claudication. Physical examination showed the level of muscle strength of his left first toe was 3/5. Images illustrated a destruction of the intervertebral space, and a retrolisthesis at L4/5 interspace and the dural sac obviously compressed.
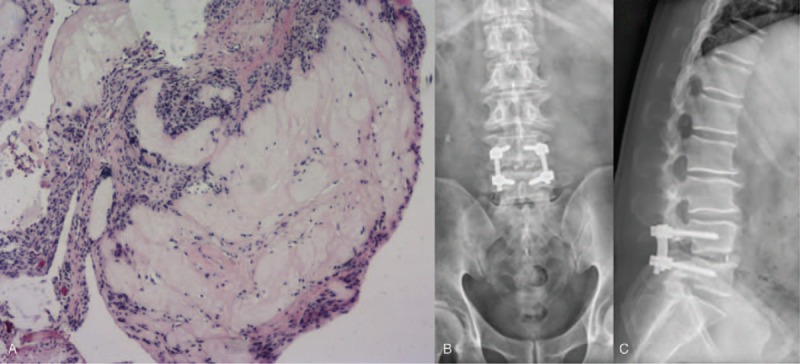
Combining with lab examinations, imaging examinations, and histopathological results, the patient was diagnosed with gouty arthritis associated with lumbar spinal stenosis, L4-5 spondylodiscitis and L4 vertebral body retrolisthesis.
The patient underwent posterior decompression, reduction, and interbody fusion, and then received an aggressive postoperative rehabilitation program.
The patient's low back pain was significantly alleviated after the operation. Postoperative X-ray shows the internal fixation was well placed and the sequence of spine was reconstructed. 12 weeks later, the lower limb symptoms of the patients were obviously improved, his muscle strength of the left first toe was 4/5, Japanese Orthopaedic Association (JOA) score was 19 and the improvement rate was 61.5%.
Gouty spondylodiscitis can cause intervertebral space instability. Sagittal imbalance and degeneration of disc with decreasing of segmental disc height are considered as the main factors of retrolisthesis. The appearance may lead to misdiagnose a patient with gout history with a destruction of the intervertebral space. Surgery is a compromise method for gouty spondylodiscitis patients with urgent neurological symptoms.
痛风主要发生在关节,但很少累及脊柱。在脊柱中,尿酸盐结晶可导致椎间隙不稳定,但很少导致椎体后滑脱。在此,我们报告一例极为罕见的痛风侵犯椎间盘并伴有腰椎椎体后滑脱的病例。
一名有痛风病史的61岁男性患者,出现严重的腰痛和间歇性跛行。体格检查显示其左拇趾肌力为3/5级。影像学检查显示椎间隙破坏,L4/5椎间隙椎体后滑脱,硬脊膜囊明显受压。
结合实验室检查、影像学检查和组织病理学结果,该患者被诊断为痛风性关节炎伴腰椎管狭窄、L4-5椎间盘炎和L4椎体后滑脱。
患者接受了后路减压、复位和椎间融合手术,术后积极进行康复训练。
术后患者腰痛明显缓解。术后X线显示内固定位置良好,脊柱序列重建。12周后,患者下肢症状明显改善,左拇趾肌力为4/5级,日本骨科学会(JOA)评分为19分,改善率为61.5%。
痛风性椎间盘炎可导致椎间隙不稳定。矢状面失衡和椎间盘退变伴节段性椎间盘高度降低被认为是椎体后滑脱的主要因素。这种表现可能导致对有痛风病史且椎间隙破坏的患者误诊。对于有紧急神经症状的痛风性椎间盘炎患者,手术是一种折中的治疗方法。