Chhatriwalla Adnan K, Decker Carole, Gialde Elizabeth, Catley Delwyn, Goggin Kathy, Jaschke Katie, Jones Philip, deBronkart Dave, Sun Tony, Spertus John A
Division of Cardiology, Saint Luke's Mid America Heart Institute, Kansas City, MO (A.K.C., C.D., E.G., K.J., P.J., J.A.S.).
Department of Medicine, Division of Cardiology, University of Missouri-Kansas City, Kansas City, MO (A.K.C., C.D., J.A.S.).
Circ Cardiovasc Qual Outcomes. 2019 Feb;12(2):e005139. doi: 10.1161/CIRCOUTCOMES.118.005139.
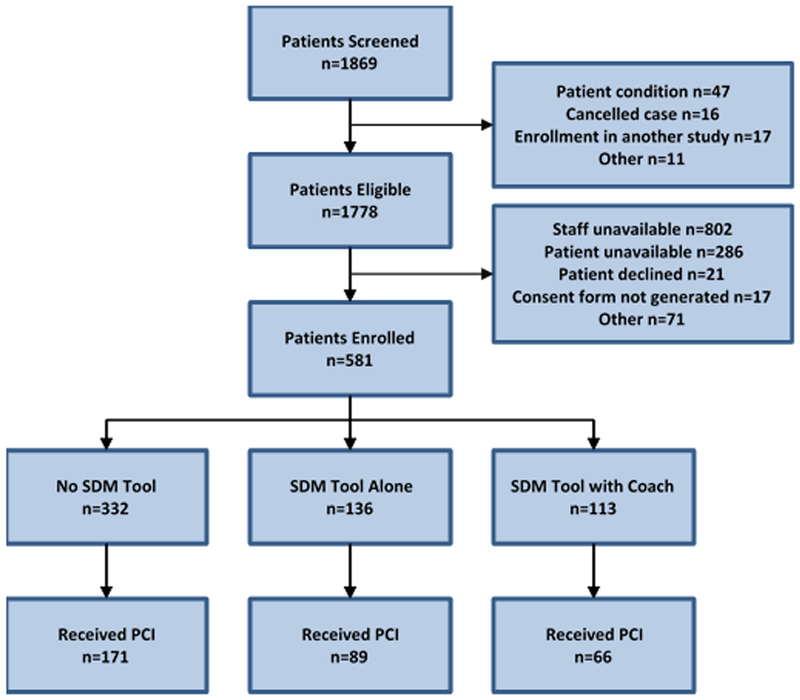
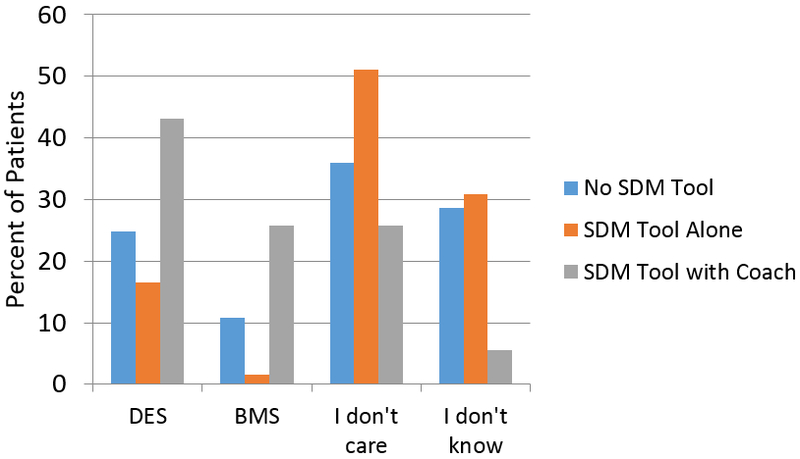
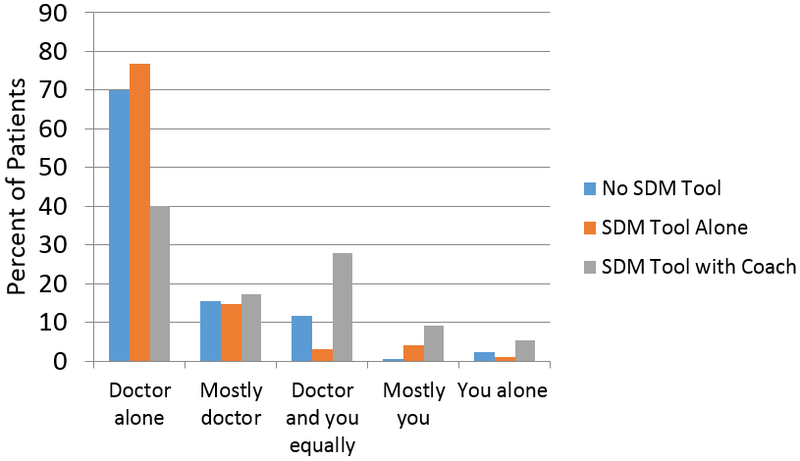
Background Drug-eluting stents reduce the risk of restenosis in patients undergoing percutaneous coronary intervention, but their use necessitates prolonged dual antiplatelet therapy, which increases costs and bleeding risk, and which may delay elective surgeries. While >80% of patients in the United States receive drug-eluting stents, less than a third report that their physicians discussed options with them. Methods and Results An individualized shared decision-making (SDM) tool for stent selection was designed and implemented at 2 US hospitals. In the postimplementation phase, all patients received the SDM tool before their procedure, with or without decision coaching from a trained nurse. All patients were interviewed with respect to their knowledge of stents, their participation in SDM, and their stent preference. Between May 2014 and December 2016, 332 patients not receiving the SDM tool, 113 receiving the SDM tool with coaching, and 136 receiving the tool without coaching were interviewed. Patients receiving the SDM tool + coaching, as compared with usual care, demonstrated higher knowledge scores (mean difference +1.8; P<0.001), reported more frequent participation in SDM (odds ratio=2.96; P<0.001), and were more likely to state a stent preference (odds ratio=2.00; P<0.001). No significant differences were observed between the use of the SDM tool without coaching and usual care. For patients who voiced a stent preference, concordance between stent desired and stent received was 98% for patients who preferred a drug-eluting stent and 50% for patients who preferred a bare metal stent. The SDM tool (with or without coaching) had no impact on stent selection or concordance. Conclusions An SDM tool for stent selection was associated with improvements in patient knowledge and SDM only when accompanied by decision coaching. However, the SDM tool (with or without coaching) had no impact on stent selection or concordance between patients' stent preference and stent received, suggesting that physician-level barriers to SDM may exist. Clinical Trial Information URL: https://www.clinicaltrials.gov . Unique Identifier: NCT02046902.
背景 药物洗脱支架可降低接受经皮冠状动脉介入治疗患者的再狭窄风险,但其使用需要延长双联抗血小板治疗,这会增加成本和出血风险,且可能延迟择期手术。在美国,超过80%的患者接受药物洗脱支架,但不到三分之一的患者报告其医生与他们讨论过选择方案。方法和结果 在美国两家医院设计并实施了一种用于支架选择的个体化共同决策(SDM)工具。在实施后阶段,所有患者在手术前都收到了SDM工具,无论是否有经过培训的护士进行决策指导。就患者对支架的了解、他们参与共同决策的情况以及他们对支架的偏好对所有患者进行了访谈。在2014年5月至2016年12月期间,对332名未收到SDM工具的患者、113名收到SDM工具并接受指导的患者以及136名收到SDM工具但未接受指导的患者进行了访谈。与常规护理相比,接受SDM工具+指导的患者知识得分更高(平均差异+1.8;P<0.001),报告参与共同决策更频繁(优势比=2.96;P<0.001),并且更有可能表明对支架的偏好(优势比=2.00;P<0.001)。在未接受指导使用SDM工具和常规护理之间未观察到显著差异。对于表达了支架偏好的患者,对于偏好药物洗脱支架的患者,期望的支架与实际接受的支架之间的一致性为98%,对于偏好裸金属支架的患者为50%。SDM工具(无论有无指导)对支架选择或一致性均无影响。结论 仅在有决策指导的情况下,用于支架选择的共同决策工具才与患者知识和共同决策的改善相关。然而,SDM工具(无论有无指导)对支架选择或患者的支架偏好与实际接受的支架之间的一致性均无影响,这表明可能存在医生层面的共同决策障碍。临床试验信息网址:https://www.clinicaltrials.gov 。唯一标识符:NCT02046902。