Department of Cardiothoracic Surgery, Stanford University, School of Medicine, Stanford, California; Department of Health and Research Policy, Stanford University, School of Medicine, Stanford, California.
The Heart Hospital Baylor Plano, Plano, Texas.
J Am Coll Cardiol. 2019 Feb 19;73(6):643-651. doi: 10.1016/j.jacc.2018.10.086.
For the management of descending thoracic aortic aneurysms, recent evidence has suggested that outcomes of open surgical repair may surpass thoracic endovascular aortic repair (TEVAR) in as early as 2 years.
The purpose of this study was to evaluate the comparative effectiveness of TEVAR and open surgical repair in the treatment of intact descending thoracic aortic aneurysms.
Using the Medicare database, a retrospective study using regression discontinuity design and propensity score matching was performed on patients with intact descending thoracic aortic aneurysms who underwent TEVAR or open surgical repair between 1999 and 2010 with follow-up through 2014. Survival was assessed with restricted mean survival time. Perioperative mortality was assessed with logistic regression. Reintervention was evaluated as a secondary outcome.
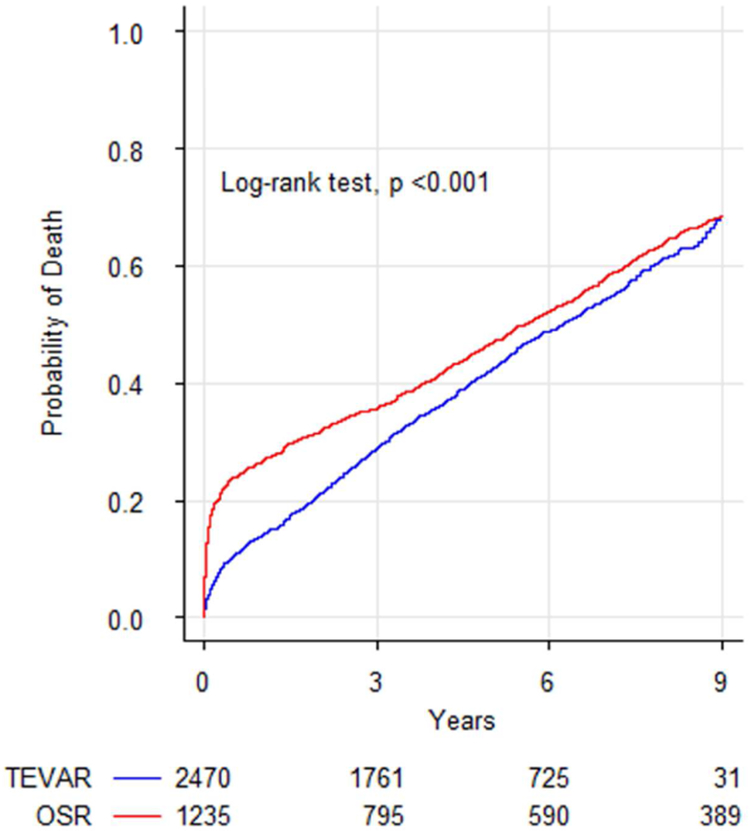
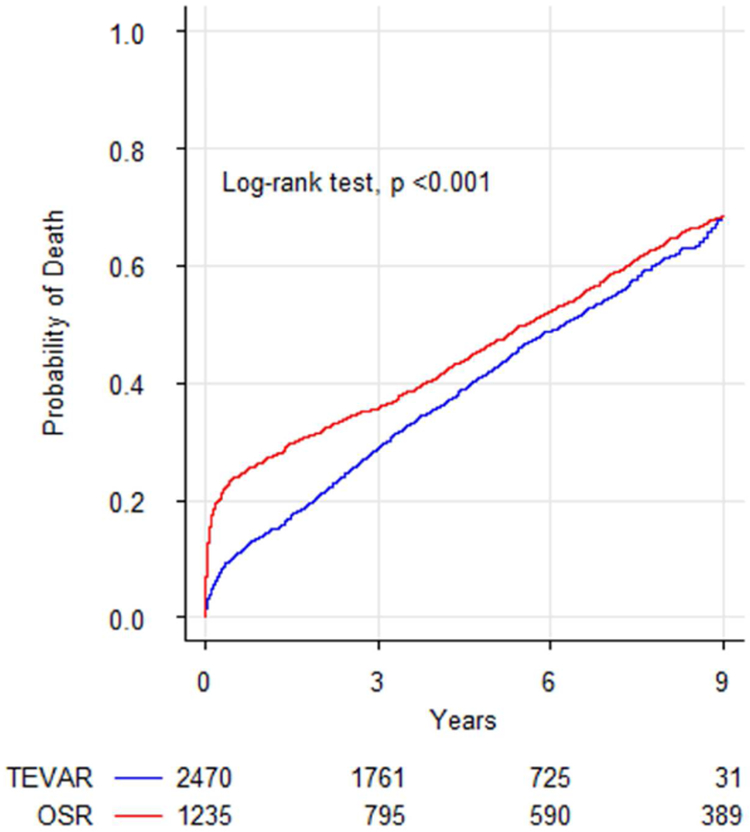
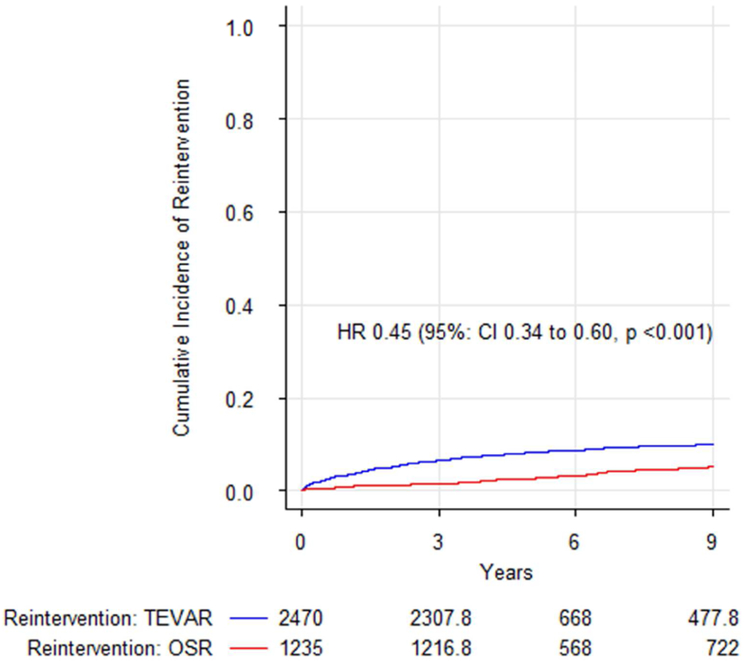
Matching created comparable groups with 1,235 open surgical repair patients matched to 2,470 TEVAR patients. The odds of perioperative mortality were greater for open surgical repair: high-volume center, odds ratio (OR): 1.97 (95% confidence interval [CI]: 1.53 to 2.61); low-volume center, OR: 3.62 (95% CI: 2.88 to 4.51). The restricted mean survival time difference favored TEVAR at 9 years, -209.2 days (95% CI: -298.7 to -119.7 days; p < 0.001) for open surgical repair. Risk of reintervention was lower for open surgical repair, hazard ratio: 0.40 (95% CI: 0.34 to 0.60; p < 0.001).
Open surgical repair was associated with increased odds of early postoperative mortality but reduced late hazard of death. Despite the late advantage of open repair, mean survival was superior for TEVAR. TEVAR should be considered the first line for repair of intact descending thoracic aortic aneurysms in Medicare beneficiaries.
对于降主动脉夹层瘤的治疗,最近的证据表明,开放手术修复的结果可能在 2 年内超过胸主动脉腔内修复术(TEVAR)。
本研究旨在评估 TEVAR 和开放手术修复在治疗完整降主动脉夹层瘤中的比较效果。
利用医疗保险数据库,对 1999 年至 2010 年间接受 TEVAR 或开放手术修复的完整降主动脉夹层瘤患者进行回顾性研究,采用回归间断设计和倾向评分匹配,并随访至 2014 年。采用限制性平均生存时间评估生存情况。采用 logistic 回归评估围手术期死亡率。将再次干预作为次要结果进行评估。
匹配后创建了具有可比性的两组患者,1235 例开放手术修复患者与 2470 例 TEVAR 患者相匹配。开放手术修复的围手术期死亡率更高:高容量中心,优势比(OR):1.97(95%置信区间[CI]:1.53 至 2.61);低容量中心,OR:3.62(95% CI:2.88 至 4.51)。TEVAR 治疗 9 年的限制性平均生存时间差为-209.2 天(95% CI:-298.7 至-119.7 天;p < 0.001),有利于 TEVAR。开放手术修复的再干预风险较低,风险比:0.40(95% CI:0.34 至 0.60;p < 0.001)。
开放手术修复与早期术后死亡率增加相关,但死亡风险降低。尽管开放修复的晚期优势明显,但 TEVAR 的平均生存时间更优。TEVAR 应被视为 Medicare 受益人的完整降主动脉夹层瘤修复的首选方法。