Elder J Bradley, Huntoon Kristin, Otero Jose, Kaya Behiye, Hatef Jeff, Eltobgy Mostafa, Lonser Russell R
Department of Neurological Surgery, The Ohio State University Wexner Medical Center, 410 West 10th Avenue, Doan 1047, Columbus, OH, 43210, USA.
Division of Neuropathology, Department of Pathology, The Ohio State University Wexner Medical Center, Columbus, OH, USA.
Diagn Pathol. 2019 Feb 15;14(1):19. doi: 10.1186/s13000-019-0794-4.
Laser-interstitial thermal therapy (LITT) has been supported by some authors as an ablative treatment of glioblastoma multiforme (GBM). Although the effects of LITT have been modeled in vivo, the histologic effects in a clinical circumstance have not been described. We analyzed tissue from a patient who underwent LITT as primary treatment for GBM.
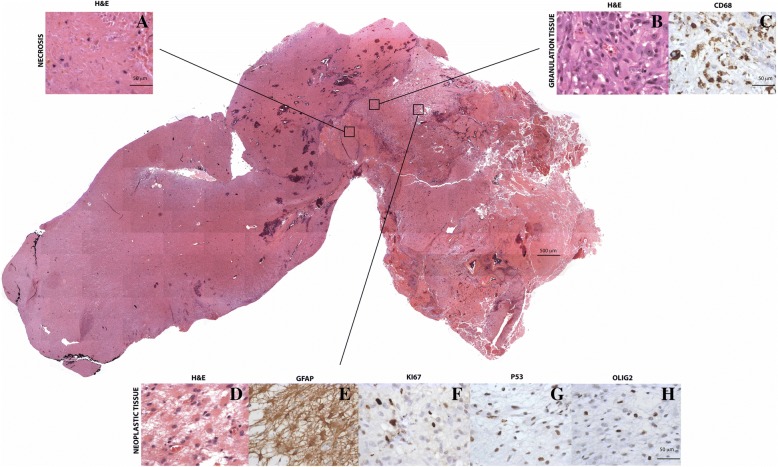
A 62-year-old male was diagnosed with a left temporal GBM and underwent LITT at an outside institution. Despite corticosteroid therapy, the patient was referred with increasing headache and acalculia associated with progressive peritumoral edema two weeks after LITT procedure. En bloc resection of the enhancing lesion and adjacent temporal lobe was performed with steroid-independent symptom resolution (follow-up, > 2 years). Histologic analysis revealed three distinct histologic zones concentrically radiating from the center of the treatment site. An acellular central region of necrosis (Zone 1) was surrounded by a rim of granulation tissue with macrophages (CD68) (Zone 2; mean thickness, 1.3 ± 0.3 mm [±S.D.]). Viable tumor cells (identified by Ki-67, p53 and Olig2 immunohistochemistry) were found (Zone 3) immediately adjacent to granulation tissue. The histologic volume of thermal tissue ablation/granulation was consistent with preoperative (pre-resection) magnetic resonance (MR)-imaging.
These findings are the first in vivo in humans to reveal that LITT causes a defined pattern of tissue necrosis, concentric destruction of tumor and tissue with viable tumor cells just beyond the zones of central necrosis and granulation. Furthermore, MR-imaging appears to be an accurate surrogate of tissue/tumor ablation in the early period (2 weeks) post-LITT treatment. Surgery is an effective strategy for patients with post-LITT swelling which does not respond to steroids.
一些作者支持激光间质热疗(LITT)作为多形性胶质母细胞瘤(GBM)的一种消融治疗方法。尽管LITT的效果已在体内进行了模拟,但尚未描述其在临床情况下的组织学效应。我们分析了一名接受LITT作为GBM主要治疗方法的患者的组织。
一名62岁男性被诊断为左颞叶GBM,并在外部机构接受了LITT治疗。尽管进行了皮质类固醇治疗,但患者在LITT手术后两周因头痛加剧和与进行性瘤周水肿相关的失算症而被转诊。对强化病变和相邻颞叶进行了整块切除,症状在停用类固醇后得到缓解(随访时间>2年)。组织学分析显示,从治疗部位中心呈同心放射状有三个不同的组织学区域。无细胞的中央坏死区域(区域1)被一层含有巨噬细胞(CD68)的肉芽组织包围(区域2;平均厚度为1.3±0.3毫米[±标准差])。在紧邻肉芽组织的区域发现了存活的肿瘤细胞(通过Ki-67、p53和Olig2免疫组织化学鉴定)(区域3)。热组织消融/肉芽组织的组织学体积与术前(切除前)磁共振(MR)成像一致。
这些发现首次在人体中揭示,LITT会导致特定模式的组织坏死,肿瘤和组织呈同心性破坏,在中央坏死和肉芽组织区域之外紧邻有存活的肿瘤细胞。此外,MR成像似乎是LITT治疗后早期(2周)组织/肿瘤消融的准确替代指标。对于LITT后肿胀且对类固醇无反应的患者,手术是一种有效的治疗策略。