Department of Health Services Research and Policy, London School of Hygiene and Tropical Medicine, London, United Kingdom.
J.E. Cairnes School of Business & Economics, National University of Ireland, Galway, Ireland.
JAMA Netw Open. 2019 Feb 1;2(2):e187704. doi: 10.1001/jamanetworkopen.2018.7704.
It is unknown which deteriorating ward patients benefit from intensive care unit (ICU) transfer.
To use an instrumental variable (IV) method that assesses heterogeneity and to evaluate estimates of person-centered treatment effects of ICU transfer and 28-day hospital mortality by age and illness severity.
DESIGN, SETTING, AND PARTICIPANTS: An analysis of a prospective cohort study from November 1, 2010, to December 31, 2011. The dates of this analysis were June 1, 2017, to June 30, 2018. The setting was a multicenter study of 49 UK National Health Service hospitals. Participants were 9192 deteriorating ward patients assessed for ICU transfer (4596 matched pairs). The study matched on baseline characteristics to strengthen the IV and to balance observed confounders between the comparison groups.
Transfer to the ICU or continued care on general wards.
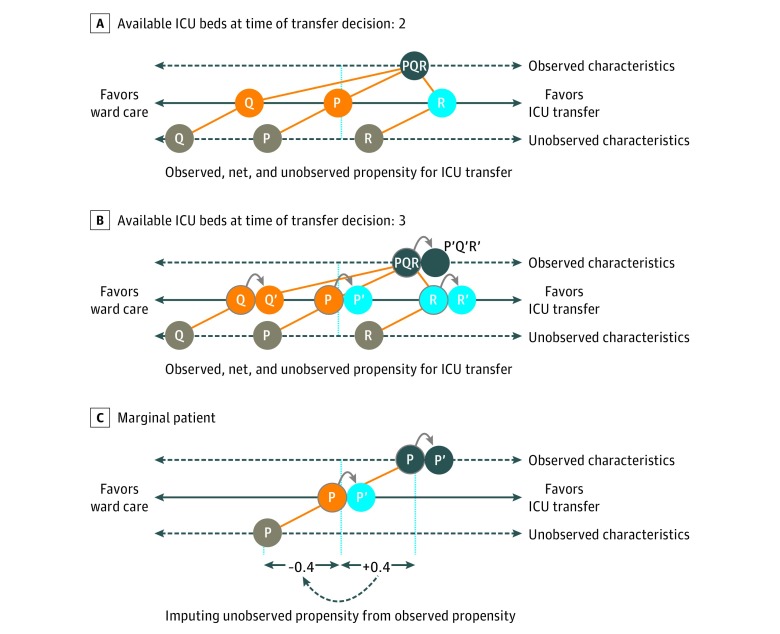
Mortality at 28 days (primary outcome) and 90 days. To address unobserved confounding, ICU bed availability was the IV for whether or not a patient was transferred. The study used the IV approach to evaluate estimates of treatment effect of ICU transfer and mortality according to age and physiological severity alone and in combination.
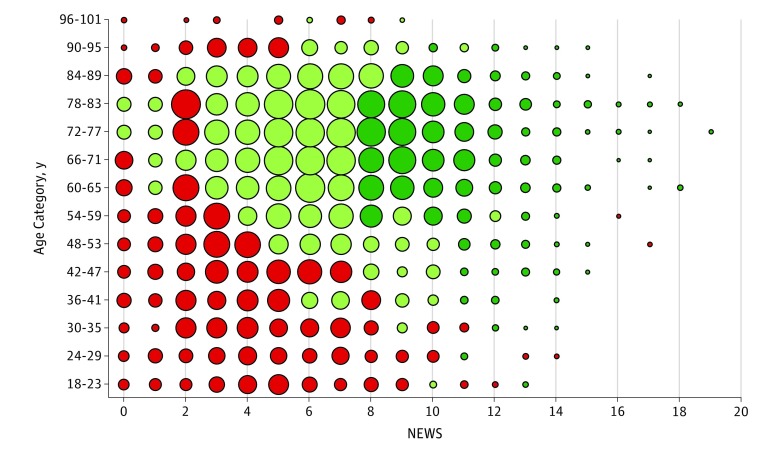
Both comparison groups included 4596 patients. In the group assessed with "many" ICU beds available (median, 7), 52.8% were male, and the mean (SD) age was 65.2 (17.7) years; in the group assessed with "few" ICU beds available (median, 2), 53.3% were male, and the mean (SD) age was 65.0 (17.3) years. The overall 28-day mortality estimates were 23.2% (2090 predicted deaths) if all of the matched patients were transferred vs 28.1% (2534 predicted deaths) if none of the matched patients were transferred, an estimated risk difference of -4.9% (95% CI, -26.4% to 16.6%). The estimated effects of ICU transfer differed by age and by physiological severity according to the National Early Warning Score (NEWS): the absolute risk differences in 28-day mortality after ICU transfer ranged from 7.7% (95% CI, -5.5% to 21.0%) for ages 18 to 23 years to -5.0% (95% CI -26.5% to 16.6%) for age 78 to 83 years and ranged from 3.7% (95% CI, -12.1% to 19.5%) for NEWS of 0 to -25.4% (95% CI, -50.6% to -0.2%) for NEWS of 19. The absolute risk differences for elderly patients (≥75 years) were -11.6% (95% CI, -39.0% to 15.8%) for those with high NEWS (>6), -4.8% (95% CI, -30.5% to 20.9%) for those with moderate NEWS (5-6), and -1.0% (95% CI, -24.8% to 22.8%) for those with low NEWS (<5). The corresponding estimates for subgroups of younger patients (<75 years) were -8.4% (95% CI, -31.0% to 14.1%), -2.1% (95% CI, -21.1% to 16.9%), and 1.4% (95% CI, -14.5% to 17.4%).
This study using a this person-centered IV approach found that the benefits of ICU care may increase among patients at high levels of baseline physiological severity across different age groups, especially among elderly patients.
重要性:尚不清楚哪些病情恶化的病房患者从 ICU 转移中受益。
目的:使用评估异质性的工具变量(IV)方法,根据年龄和疾病严重程度评估 ICU 转移和 28 天医院死亡率的个体中心治疗效果的估计值。
设计、地点和参与者:这是一项从 2010 年 11 月 1 日至 2011 年 12 月 31 日的前瞻性队列研究的分析。该分析的日期为 2017 年 6 月 1 日至 2018 年 6 月 30 日。该研究在英国 49 家 NHS 医院进行。研究对象为 9192 名接受 ICU 转移评估的病情恶化病房患者(4596 对匹配)。研究采用匹配基线特征的方法来加强 IV,并在比较组之间平衡观察到的混杂因素。
暴露:转至 ICU 或继续在普通病房接受治疗。
主要结果和测量:28 天(主要结果)和 90 天死亡率。为了解决未观察到的混杂因素,可用 ICU 床位数量是患者是否转移的 IV。该研究使用 IV 方法根据年龄和生理严重程度单独和组合评估 ICU 转移和死亡率的治疗效果估计值。
结果:两组比较组均包括 4596 名患者。在评估“有很多”ICU 床位可用的组(中位数为 7)中,52.8%为男性,平均(SD)年龄为 65.2(17.7)岁;在评估“有很少”ICU 床位可用的组(中位数为 2)中,53.3%为男性,平均(SD)年龄为 65.0(17.3)岁。如果所有匹配的患者都转移,28 天死亡率的总估计值为 23.2%(2090 例预测死亡);如果没有转移,28 天死亡率的估计值为 28.1%(2534 例预测死亡),估计风险差异为-4.9%(95%CI,-26.4%至 16.6%)。根据国家早期预警评分(NEWS),ICU 转移的效果因年龄和生理严重程度而异:ICU 转移后 28 天死亡率的绝对风险差异范围为 18 至 23 岁年龄组的 7.7%(95%CI,-5.5%至 21.0%)至 78 至 83 岁年龄组的-5.0%(95%CI,-26.5%至 16.6%),从 0 至-25.4%(95%CI,-50.6%至-0.2%)的 NEWS 范围为-3.7%(95%CI,-12.1%至 19.5%)。对于年龄较大(≥75 岁)的老年患者,高 NEWS(>6)患者的绝对风险差异为-11.6%(95%CI,-39.0%至 15.8%),中 NEWS(5-6)患者为-4.8%(95%CI,-30.5%至 20.9%),低 NEWS(<5)患者为-1.0%(95%CI,-24.8%至 22.8%)。年龄较小(<75 岁)的亚组患者的相应估计值为-8.4%(95%CI,-31.0%至 14.1%)、-2.1%(95%CI,-21.1%至 16.9%)和 1.4%(95%CI,-14.5%至 17.4%)。
结论和相关性:本研究使用个体中心 IV 方法发现,ICU 护理的益处可能会在不同年龄组中高基线生理严重程度的患者中增加,尤其是老年患者。