Xia Dao-Kui, Hu Zhi-Gang, Tian Yu-Feng, Zeng Fan-Jun
Department of Thoracic Surgery, Yichang Central People's Hospital, Yichang, PR China.
Department of Respiratory Medicine, Respiratory Disease Research Institute of China, Three Gorges University, Yichang, PR China,
Drug Des Devel Ther. 2019 Jan 23;13:405-422. doi: 10.2147/DDDT.S187690. eCollection 2019.
Previous clinical studies reported inconsistent results on the associations of statins with the mortality and survival of lung cancer patients. This review and meta-analysis summarized the impact of statins on mortality and survival of lung cancer patients.
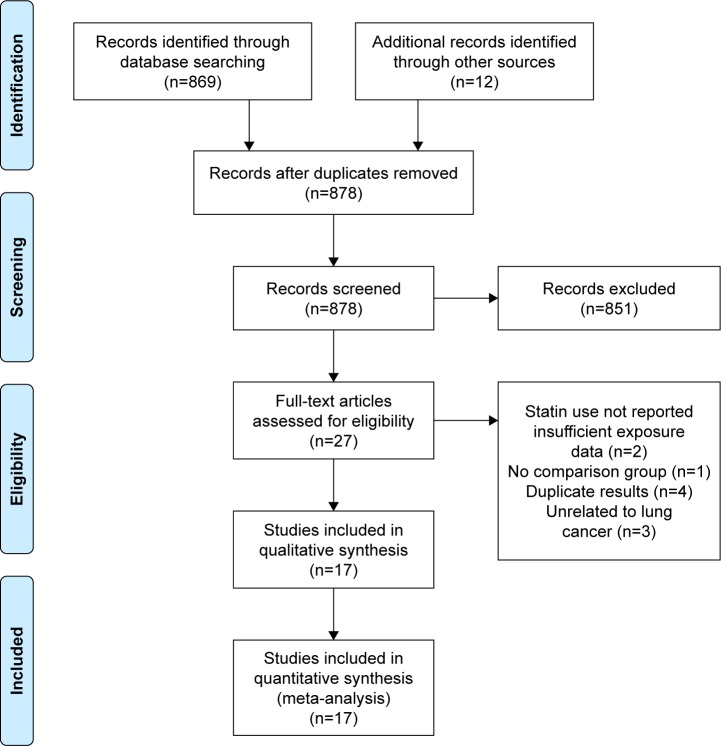
Eligible papers of this meta-analysis were searched by using PubMed, EMBASE, and Cochrane until July 2017. Primary end points were the mortality (all-cause mortality and cancer-specific mortality) and survival (progression-free survival and overall survival) of patients with statin use. Secondary end points were overall response rate and safety. The random-effects model was used to calculate pooled HRs and 95% CIs.
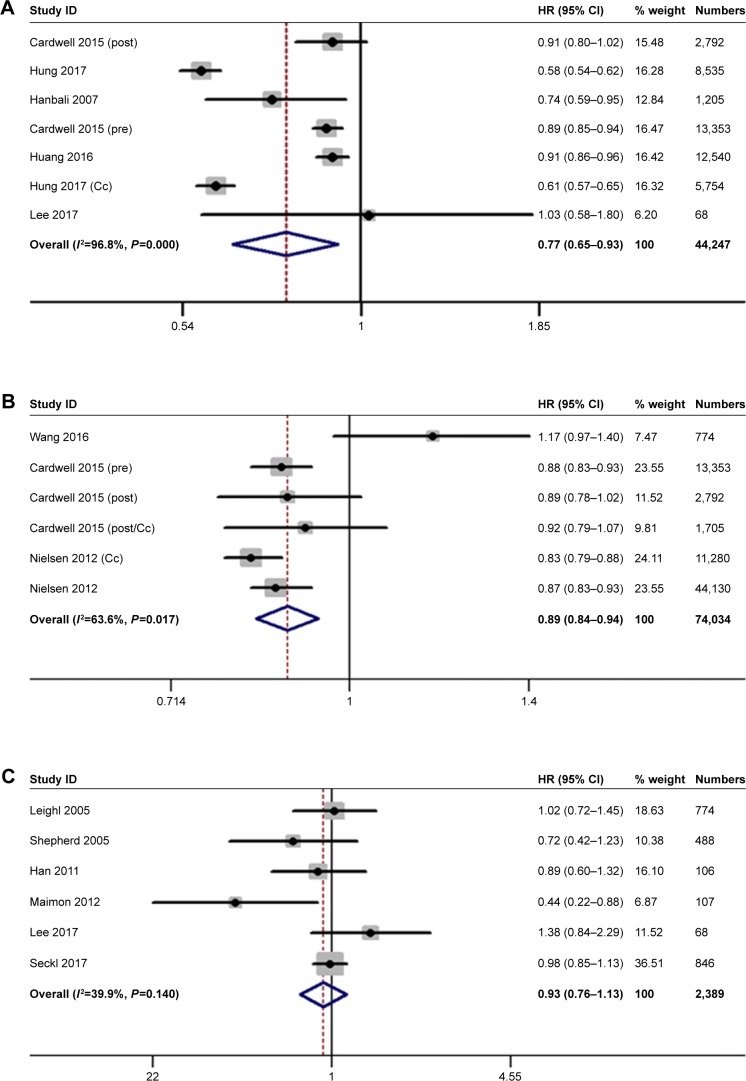
Seventeen studies involving 98,445 patients were included in the meta-analysis. In observational studies, the pooled HR indicated that statins potentially decreased the cancer-specific mortality and promoted the overall survival of lung cancer patients. Statins showed an association with decreased all-cause mortality in cohort studies (HR =0.77, 95% CI: 0.59-0.99), but not in case-control studies (HR =0.75, 95% CI: 0.50-1.10). However, statin use showed no impact on mortality and overall survival in randomized controlled trials. Meanwhile, this meta-analysis indicated that statin use did not affect the progression-free survival of lung cancer patients in observational studies and randomized controlled trials. In addition, statins potentially enhanced the effects of tyrosine kinase inhibitors (HR=0.86, 95% CI: 0.76-0.98) and chemotherapy (HR=0.86, 95% CI: 0.81-0.91) on the overall survival of patients with non-small-cell lung cancer, but did not increase overall response rate and toxicity.
Statins were potentially associated with the decreasing risk of mortality and the improvement of overall survival in observational studies but not in randomized controlled trials.
先前的临床研究报告了他汀类药物与肺癌患者死亡率和生存率之间关联的不一致结果。本综述和荟萃分析总结了他汀类药物对肺癌患者死亡率和生存率的影响。
使用PubMed、EMBASE和Cochrane检索截至2017年7月符合条件的本荟萃分析论文。主要终点是使用他汀类药物患者的死亡率(全因死亡率和癌症特异性死亡率)和生存率(无进展生存期和总生存期)。次要终点是总缓解率和安全性。采用随机效应模型计算合并风险比(HR)和95%置信区间(CI)。
荟萃分析纳入了17项研究,涉及98445名患者。在观察性研究中,合并HR表明他汀类药物可能降低癌症特异性死亡率并提高肺癌患者的总生存期。他汀类药物在队列研究中显示与全因死亡率降低有关(HR = 0.77,95% CI:0.59 - 0.99),但在病例对照研究中未显示(HR = 0.75,95% CI:0.50 - 1.10)。然而,在随机对照试验中,使用他汀类药物对死亡率和总生存期没有影响。同时,本荟萃分析表明,在观察性研究和随机对照试验中,使用他汀类药物不影响肺癌患者的无进展生存期。此外,他汀类药物可能增强酪氨酸激酶抑制剂(HR = 0.86,95% CI:0.76 - 0.98)和化疗(HR = 0.86,95% CI:0.81 - 0.91)对非小细胞肺癌患者总生存期的影响,但未增加总缓解率和毒性。
在观察性研究中,他汀类药物可能与降低死亡风险和改善总生存期有关,但在随机对照试验中并非如此。