Urwyler Pascal, Abu Hussein Nebal, Bridevaux Pierre O, Chhajed Prashant N, Geiser Thomas, Grendelmeier Peter, Joos Zellweger Ladina, Kohler Malcolm, Maier Sabrina, Miedinger David, Tamm Michael, Thurnheer Robert, Dieterle Thomas, Leuppi Joerg D
1University Clinic of Medicine, Cantonal Hospital Baselland, University of Basel, Rheinstrasse 26, 4410 Liestal, Switzerland.
2University Hospital Basel, University of Basel, Spitalstrasse 21, 4031 Basel, Switzerland.
Multidiscip Respir Med. 2019 Feb 5;14:7. doi: 10.1186/s40248-019-0168-5. eCollection 2019.
The Swiss COPD cohort was established in 2006 to collect data in a primary care setting. The objective of this study was to evaluate possible predictive factors for exacerbation and re-exacerbation.
In order to predict exacerbation until the next visit based on the knowledge of exacerbation since the last visit, a multistate model described by Therneau and Grambsch was performed.
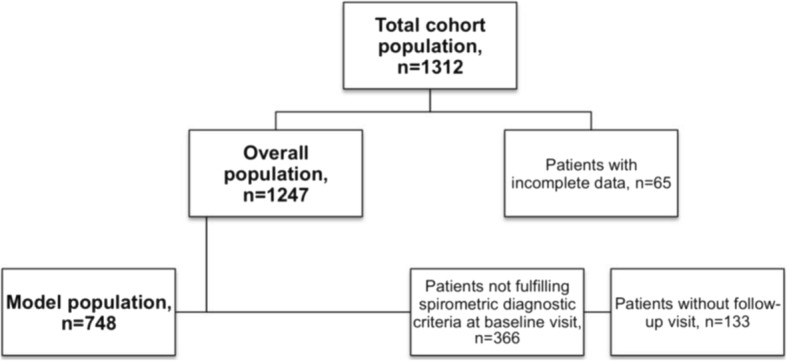
Data of 1,247 patients (60.4% males, 46.6% current smokers) were analyzed, 268 (21.5%) did not fulfill spirometric diagnostic criteria for COPD. Data of 748 patients (63% males, 44.1% current smokers) were available for model analysis. In order to predict exacerbation an extended Cox Model was performed. Mean FEV/FVC-ratio was 53.1% (±11.5), with a majority of patients in COPD GOLD classes 2 or 3. Hospitalization for any reason (HR1.7; = 0.04) and pronounced dyspnea (HR for mMRC grade four 3.0; < 0.001) at most recent visit as well as prescription of short-acting bronchodilators (HR1.7; < 0.001), inhaled (HR1.2; = 0.005) or systemic corticosteroids (HR1.8; = 0.015) were significantly associated with exacerbation when having had no exacerbation at most recent visit. Higher FEV/FVC (HR0.9; = 0.008) and higher FEV values (HR0.9; = 0.001) were protective. When already having had an exacerbation at the most recent visit, pronounced dyspnea (HR for mMRC grade 4 1.9; = 0.026) and cerebrovascular insult (HR2.1; = 0.003) were significantly associated with re-exacerbation. Physical activity (HR0.6; = 0.031) and treatment with long-acting anticholinergics (HR0.7; = 0.044) seemed to play a significant protective role. In a best subset model for exacerbation, higher FEV significantly reduced and occurrence of sputum increased the probability of exacerbation. In the same model for re-exacerbation, coronary heart disease increased and hospitalization at most recent visit seemed to reduce the risk for re-exacerbation.
Our data confirmed well-established risk factors for exacerbations whilst analyzing their predictive association with exacerbation and re-exacerbation. This study confirmed the importance of spirometry in primary care, not only for diagnosis but also as a risk evaluation for possible future exacerbations.
Our study got approval by local ethical committee in 2006 (EK Nr. 170/06) and was registered retrospectively on ClinicalTrials.gov (NCT02065921, 19 of February 2014).
瑞士慢性阻塞性肺疾病(COPD)队列于2006年建立,旨在收集初级医疗环境中的数据。本研究的目的是评估加重和再次加重的可能预测因素。
为了根据自上次就诊以来的加重情况预测直至下次就诊时的加重情况,采用了由Therneau和Grambsch描述的多状态模型。
分析了1247例患者的数据(男性占60.4%,当前吸烟者占46.6%),其中268例(21.5%)不符合COPD的肺量计诊断标准。748例患者(男性占63%,当前吸烟者占44.1%)的数据可用于模型分析。为了预测加重情况,进行了扩展的Cox模型分析。平均FEV/FVC比值为53.1%(±11.5),大多数患者属于慢性阻塞性肺疾病全球倡议(GOLD)2级或3级。在最近一次就诊时,因任何原因住院(风险比[HR]1.7;P = 0.04)、明显呼吸困难(mMRC 4级的HR为3.0;P < 0.001)以及使用短效支气管扩张剂(HR1.7;P < 0.001)、吸入(HR1.2;P = 0.005)或全身用糖皮质激素(HR1.8;P = 0.015)在最近一次就诊时无加重的情况下与加重显著相关。较高的FEV/FVC(HR0.9;P = 0.008)和较高的FEV值(HR0.9;P = 0.001)具有保护作用。当最近一次就诊时已经发生过加重时,明显呼吸困难(mMRC 4级的HR为1.9;P = 0.026)和脑血管损伤(HR2.1;P = 0.003)与再次加重显著相关。身体活动(HR0.6;P = 0.031)和长效抗胆碱能药物治疗(HR0.7;P = 0.044)似乎起到显著的保护作用。在加重情况的最佳子集模型中,较高的FEV显著降低,痰液出现增加了加重的可能性。在同一再次加重模型中,冠心病增加,最近一次就诊时住院似乎降低了再次加重的风险。
我们的数据在分析加重及再次加重的预测关联时证实了已确立的加重风险因素。本研究证实了肺量计在初级医疗中的重要性,不仅用于诊断,还作为未来可能加重情况的风险评估。
我们的研究于2006年获得当地伦理委员会批准(伦理委员会编号170/06),并于2014年2月19日在ClinicalTrials.gov上进行了回顾性注册(NCT02065921)。