Animal Research Unit, BioCruces Bizkaia Health Research Institute, Barakaldo, Bizkaia, Spain.
Medical Devices Group, University of Basque Country, Portugalete, Bizkaia, Spain.
Pediatr Pulmonol. 2019 May;54(5):644-654. doi: 10.1002/ppul.24277. Epub 2019 Feb 18.
Nasal continuous-positive airway pressure (nCPAP) with the INSURE (INtubation-SURfactant-Extubation) or LISA (Less-Invasive Surfactant Administration) procedures are increasingly being chosen as the initial treatment for neonates with surfactant deficiency. Our objective was to compare the effects on cerebral oxygenation of different methods for surfactant administration: INSURE and LISA, using a nasogastric tube (NT) or a LISAcath® catheter, in spontaneously breathing SF-deficient newborn piglets.
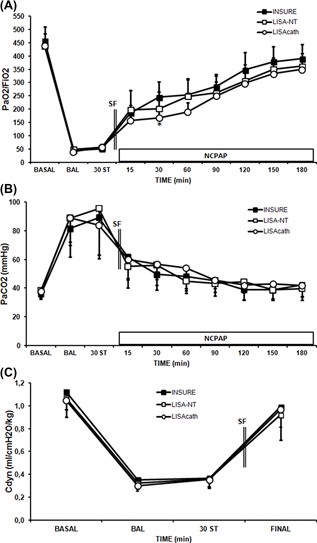
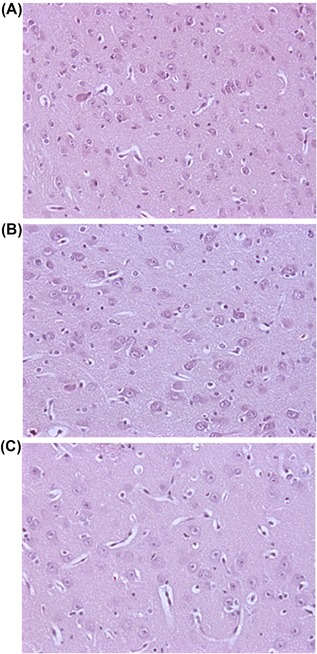
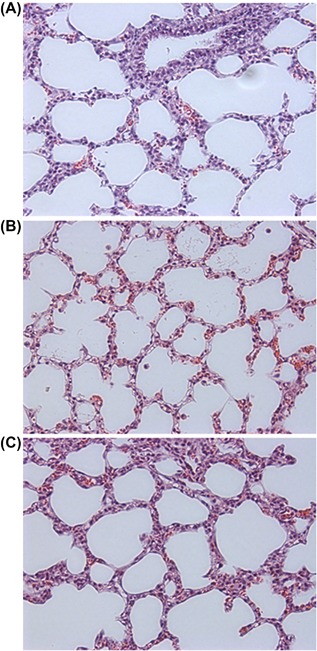
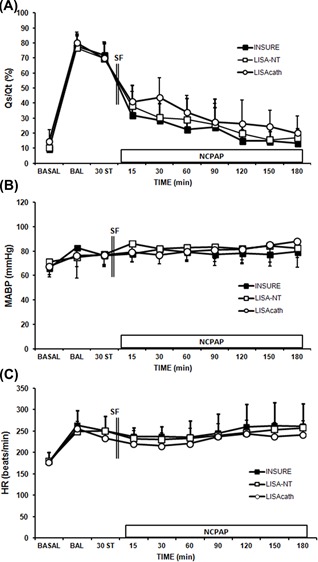
Eighteen newborn piglets with SF-deficient lung injury produced by repetitive bronchoalveolar lavages were randomly assigned to INSURE, LISA-NT, or LISAcath® groups. We assessed pulmonary (gas exchange, lung mechanics, lung histology) and hemodynamic (mean arterial blood pressure, heart rate) changes, cerebral oxygenation (cTOI) and cerebral fractional tissue extraction (cFTOE), with near-infrared spectroscopy, carotid blood flow and brain histology.
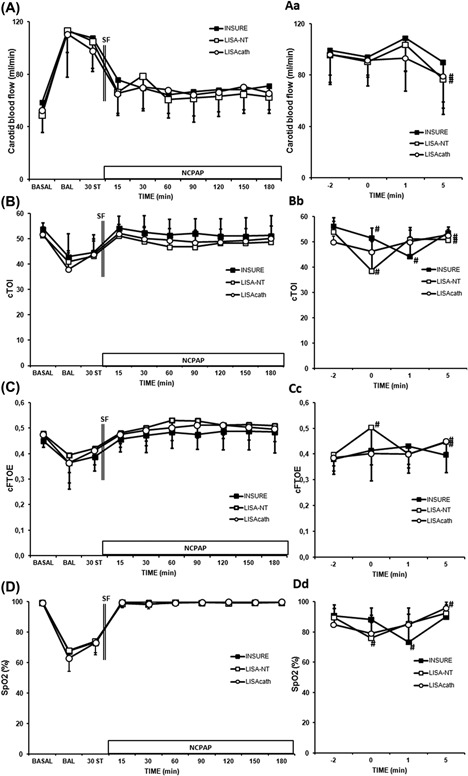
SF-deficient piglets developed respiratory distress (F = 1, pH <7.2, P >70 mmHg, P <70 mmHg, C <0.5 mL/cmH O/kg). Rapid improvements in pulmonary status were observed in all surfactant-treated groups without hemodynamic alterations. In the INSURE group, a transient decrease in cTOI occurred during and immediately after surfactant administration, while cTOI only decreased during surfactant administration in the LISA-NT group and did not change significantly in the LISAcath® group. Brain injury scores were low in all surfactant-treated groups.
In spontaneously breathing SF-deficient newborn piglets, short-lasting decreases in cerebral oxygenation are associated with surfactant administration by the INSURE method or LISA using an NT, while no cerebral oxygenation changes occurred with LISA using a LISAcath®. Notably, none of treatments studied seems to have a negative impact on the neonatal brain.
经鼻持续气道正压通气(nCPAP)联合 INSURE(插管-表面活性剂-拔管)或 LISA(经鼻气道内给予表面活性剂)程序,越来越多地被作为肺表面活性物质缺乏的新生儿初始治疗选择。我们的目的是比较不同肺表面活性物质给药方法对脑氧合的影响:INSURE 和 LISA,分别采用鼻胃管(NT)或 LISAcath®导管,在自然呼吸 SF 缺乏的新生猪模型中。
18 只通过重复支气管肺泡灌洗导致肺表面活性物质缺乏性肺损伤的新生猪随机分配到 INSURE、LISA-NT 或 LISAcath®组。我们评估了肺(气体交换、肺力学、肺组织学)和血流动力学(平均动脉血压、心率)变化,用近红外光谱仪评估脑氧合(cTOI)和脑组织提取分数(cFTOE),以及颈总动脉血流和脑组织学。
SF 缺乏的猪只出现呼吸窘迫(F = 1,pH <7.2,P >70mmHg,P <70mmHg,C <0.5mL/cmH 2 O/kg)。所有表面活性剂治疗组均未出现血流动力学改变,肺功能迅速改善。在 INSURE 组,表面活性剂给药过程中及给药后即刻 cTOI 短暂降低,而 LISA-NT 组仅在表面活性剂给药过程中 cTOI 降低,LISAcath®组无明显变化。所有接受表面活性剂治疗的组的脑损伤评分均较低。
在自然呼吸 SF 缺乏的新生猪中,INSURE 方法或使用 NT 的 LISA 进行表面活性剂给药时,脑氧合短暂下降,而使用 LISAcath®的 LISA 时则无脑氧合变化。值得注意的是,研究中没有一种治疗方法似乎对新生儿大脑有负面影响。