Section of Investigative Medicine, Division of Diabetes, Endocrinology and Metabolism, Imperial College London, 6th Floor, Commonwealth Building, Du Cane Road, London, W12 0NN, UK.
Department of Endocrinology and Nutrition, Clínica Universidad de Navarra, Pamplona, Spain.
J Transl Med. 2019 Feb 18;17(1):48. doi: 10.1186/s12967-019-1787-5.
Obesity is associated with impaired glucose tolerance which is a risk factor for cardiovascular risk. However, the oral glucose tolerance test (OGTT) is not usually performed in patients with normal fasting glycaemia, thus offering false reassurance to patients with overweight or obesity who may have post-prandial hyperglycaemia. As an alternative to resource demanding OGTTs, we aimed to examine the predictive value of anthropometric measures of total and central fat distribution for post-prandial hyperglycaemia in patients with overweight and obesity with normal fasting glycaemia enrolled in the DICAMANO study.
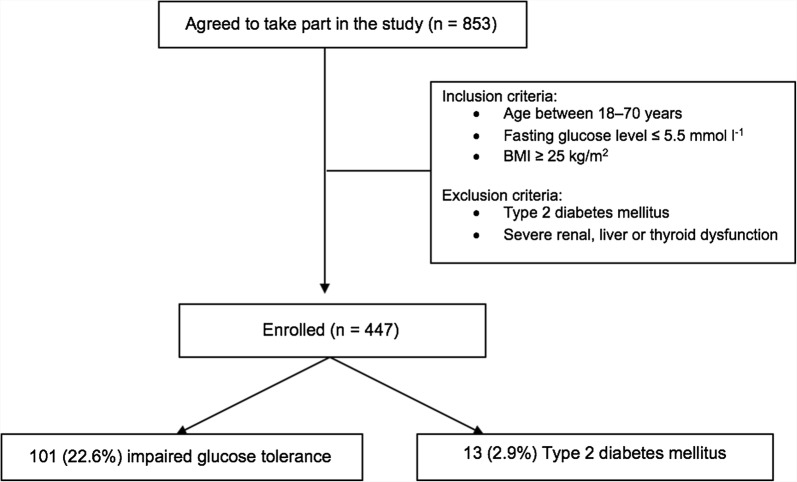
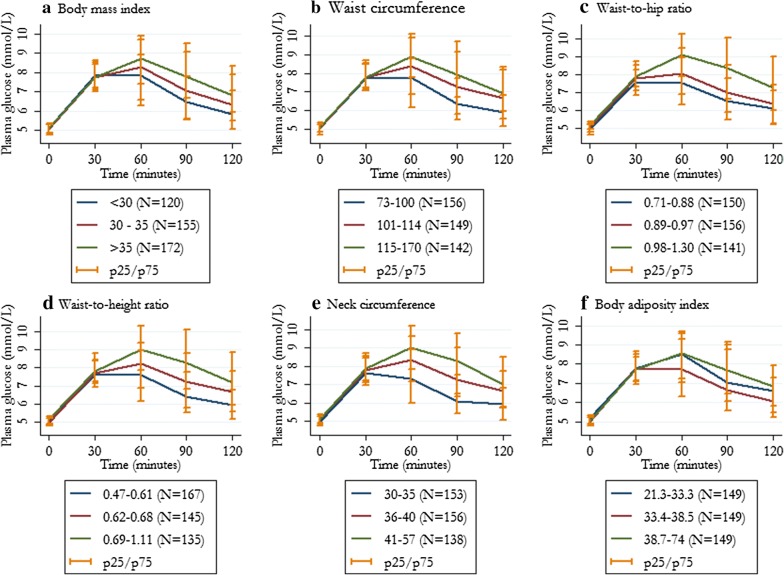
We studied 447 subjects with overweight/obesity with a fasting glucose value ≤ 5.5 mmol l (99 mg dl) and BMI ≥ 25 kg/m who underwent a 75-g OGTT. Post-prandial hyperglycaemia was defined as a glucose level ≥ 7.8 mmol l (140 mg dl) 2-h after the OGTT. The anthropometric measurements included body mass index, body adiposity index, waist circumference, neck circumference, waist-to-hip ratio and waist-to-height ratio.
The prevalence of post-prandial hyperglycaemia was 26%. Mean 1-h OGTT glucose levels, insulin resistance and beta cell dysfunction was higher in those subjects in the highest tertile for each anthropometric measurement, irrespective of fasting glucose level. Central fat depot anthropometric measurements were strongly and independently associated with an increased risk of post-prandial hyperglycaemia. After multivariable-adjustment for fasting plasma glucose level, smoking, and physical activity level, the odds ratio (95% confidence intervals) for the presence of post-prandial hyperglycaemia for neck circumference, waist circumference and waist-to-height ratio were 3.3 (1.4, 7.7), 2.4 (1.4, 4.4) and 2.5 (1.4, 4.5), respectively.
In this large and comprehensively phenotyped cohort, one in four subjects had post-prandial hyperglycaemia despite normal fasting glycaemia. Anthropometric indices of central fat distribution were strongly and independently associated with an increased risk of post-prandial hyperglycaemia. These results support the association between central adiposity and glucose derangements and demonstrate the clinical usefulness of anthropometric measurements as screening tools for the selection of patients who are most likely to benefit from an OGTT. Trial registration ClinicalTrials.gov Identifier: NCT03506581. Registered 24 April 2018-Retrospectively registered, https://clinicaltrials.gov/ct2/show/NCT03506581.
肥胖与葡萄糖耐量受损有关,葡萄糖耐量受损是心血管风险的一个危险因素。然而,对于空腹血糖正常的患者,通常不进行口服葡萄糖耐量试验(OGTT),这给超重或肥胖患者带来了错误的安慰,这些患者可能存在餐后高血糖。为了替代资源需求较高的 OGTT,我们旨在检查超重和肥胖患者中,总脂肪和中央脂肪分布的人体测量指标对空腹血糖正常的 DICAMANO 研究中患者的餐后高血糖的预测价值。
我们研究了 447 名空腹血糖值≤5.5mmol/l(99mg/dl)和 BMI≥25kg/m2 的超重/肥胖患者,他们接受了 75g OGTT。餐后高血糖定义为 OGTT 后 2 小时血糖值≥7.8mmol/l(140mg/dl)。人体测量指标包括体重指数、身体脂肪指数、腰围、颈围、腰臀比和腰高比。
餐后高血糖的患病率为 26%。无论空腹血糖水平如何,在每个人体测量指标的最高三分位组中,1 小时 OGTT 葡萄糖水平、胰岛素抵抗和β细胞功能障碍均较高。中央脂肪库人体测量指标与餐后高血糖风险增加呈强烈和独立相关。在校正空腹血浆葡萄糖水平、吸烟和体力活动水平后,颈围、腰围和腰高比的餐后高血糖存在的比值比(95%置信区间)分别为 3.3(1.4,7.7)、2.4(1.4,4.4)和 2.5(1.4,4.5)。
在这项大型、全面表型研究中,尽管空腹血糖正常,但四分之一的患者仍存在餐后高血糖。中央脂肪分布的人体测量指标与餐后高血糖风险增加密切相关。这些结果支持了中心性肥胖与葡萄糖紊乱之间的关联,并证明了人体测量作为 OGTT 选择最有可能受益的患者的筛选工具的临床实用性。
ClinicalTrials.gov 标识符:NCT03506581。2018 年 4 月 24 日注册-回顾性注册,https://clinicaltrials.gov/ct2/show/NCT03506581。