Wamil Malgorzata, Borlotti Alessandra, Liu Dan, Briosa E Gala André, Bracco Alessia, Alkhalil Mohammad, De Maria Giovanni Luigi, Piechnik Stefan K, Ferreira Vanessa M, Banning Adrian P, Kharbanda Rajesh K, Neubauer Stefan, Choudhury Robin P, Channon Keith M, Dall'Armellina Erica
Division of Cardiovascular Medicine, Radcliffe Department of Medicine, John Radcliffe Hospital, University of Oxford, Oxford, OX3 9DU, UK.
NIHR Oxford Biomedical Research Centre, John Radcliffe Hospital, Oxford, OX3 9DU, UK.
Int J Cardiovasc Imaging. 2019 Jul;35(7):1297-1308. doi: 10.1007/s10554-019-01542-8. Epub 2019 Feb 16.
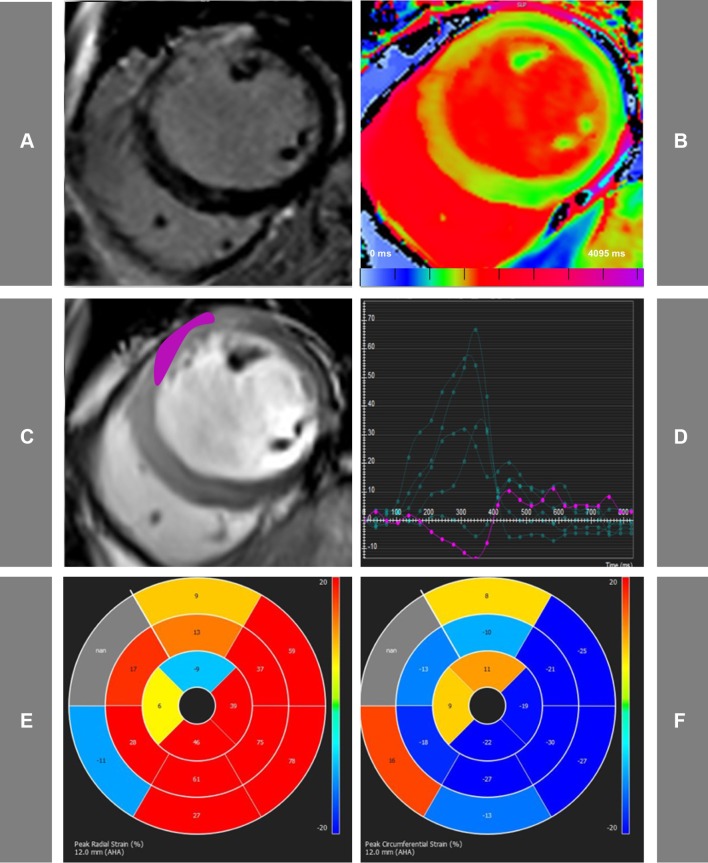
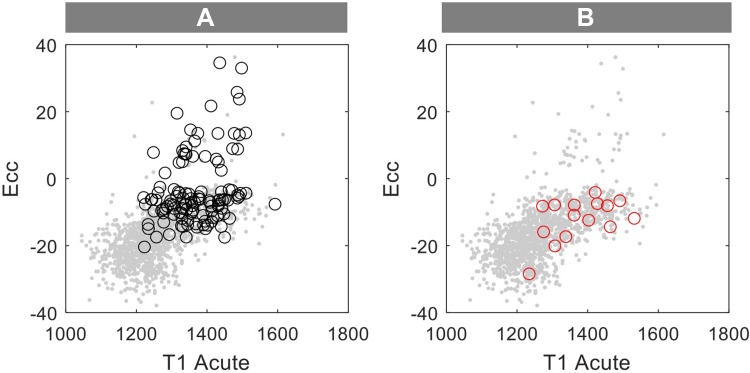
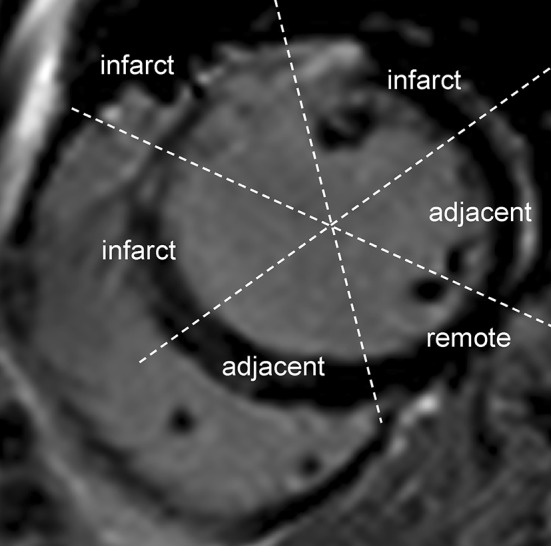
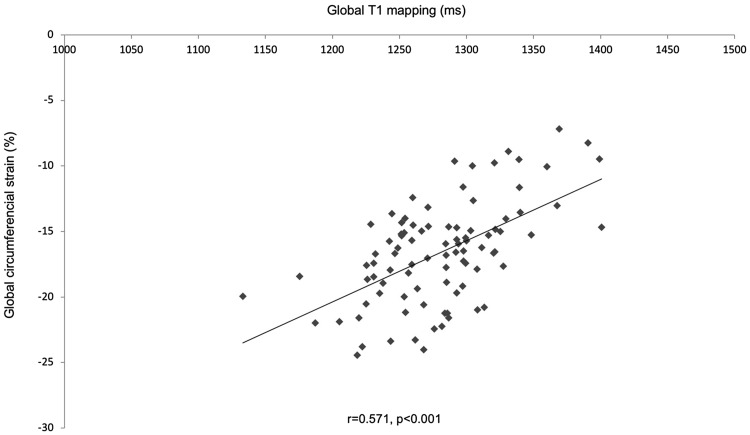
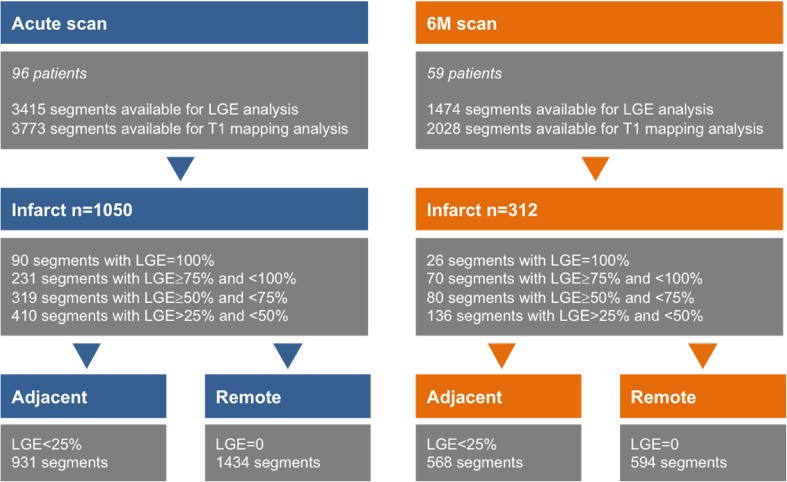
Early risk stratification after ST-segment-elevation myocardial infarction (STEMI) is of major clinical importance. Strain quantifies myocardial deformation and can demonstrate abnormal global and segmental myocardial function in acute ischaemia. Native T1-mapping allows assessment of the severity of acute ischemic injury, however its clinical applicability early post MI is limited by the complex dynamic changes happening in the myocardium post MI. We aimed to explore relationship between T1-mapping and feature tracking imaging, to establish whether combined analysis of these parameters could predict recovery after STEMI. 96 STEMI patients (aged 60 ± 11) prospectively recruited in the Oxford Acute Myocardial Infarction (OxAMI) study underwent 3T-CMR scans acutely (within 53 ± 32 h from primary percutaneous coronary intervention) and at 6 months (6M). The imaging protocol included: cine, ShMOLLI T1-mapping and late gadolinium enhancement (LGE). Segments were divided in the infarct, adjacent and remote zones based on the presence of LGE. Peak circumferential (Ecc) and radial (Err) strain was assessed using cvi42 software. Acute segmental strain correlated with segmental T1-mapping values (T1 vs. Err - 0.75 ± 0.25, p < 0.01; T1 vs. Ecc 0.72 ± 0.32, p < 0.01) and with LGE segmental injury (LGE vs. Err - 0.56 ± 0.29, p < 0.01; LGE vs. Ecc 0.54 ± 0.35, p < 0.01). Moreover, acute segmental T1 and strain predicted segmental LGE transmurality on 6M scans (p < 0.001, r = 0.5). Multiple regression analysis confirmed combined analysis of global Ecc and T1-mapping was significantly better than either method alone in predicting final infarct size at 6M (r = 0.556 vs r = 0.473 for global T1 only and r = 0.476 for global Ecc only, p < 0.001). This novel CMR method combining T1-mapping and feature tracking analysis of acute CMR scans predicts LGE transmurality and infarct size at 6M following STEMI.
ST段抬高型心肌梗死(STEMI)后的早期风险分层具有重要的临床意义。应变可量化心肌变形,并能在急性缺血时显示整体和节段性心肌功能异常。心肌组织T1加权成像可评估急性缺血损伤的严重程度,然而其在心肌梗死后早期的临床应用受到心肌梗死后心肌复杂动态变化的限制。我们旨在探讨T1加权成像与特征追踪成像之间的关系,以确定这些参数的联合分析是否能够预测STEMI后的恢复情况。在牛津急性心肌梗死(OxAMI)研究中前瞻性招募的96例STEMI患者(年龄60±11岁)在急性期(在直接经皮冠状动脉介入治疗后53±32小时内)和6个月时接受了3T心脏磁共振成像(CMR)扫描。成像方案包括:电影成像、ShMOLLI T1加权成像和延迟钆增强(LGE)。根据LGE的存在将节段分为梗死区、相邻区和远隔区。使用cvi42软件评估峰值圆周应变(Ecc)和径向应变(Err)。急性节段应变与节段T1加权成像值相关(T1与Err -0.75±0.25,p<0.01;T1与Ecc 0.72±0.32,p<0.01),并与LGE节段损伤相关(LGE与Err -0.56±0.29,p<0.01;LGE与Ecc 0.54±0.35,p<0.01)。此外,急性节段T1加权成像和应变可预测6个月扫描时节段LGE透壁性(p<0.001,r=0.5)。多元回归分析证实,在预测6个月时的最终梗死面积方面,整体Ecc和T1加权成像的联合分析明显优于单独使用任何一种方法(整体T1单独分析时r=0.556,整体Ecc单独分析时r=0.473,仅整体Ecc时r=0.476,p<0.001)。这种将T1加权成像与急性CMR扫描的特征追踪分析相结合的新型CMR方法可预测STEMI后6个月时的LGE透壁性和梗死面积。