Boyce Louis, Prasad Anoop, Barrett Matthew, Dawson-Bowling Sebastian, Millington Steven, Hanna Sammy A, Achan Pramod
Barts and the London School of Medicine and Dentistry, Whitechapel, London, E1 2AD, UK.
Royal London Hospital, Barts Health NHS Trust, Whitechapel, London, E1 1BB, UK.
Arch Orthop Trauma Surg. 2019 Apr;139(4):553-560. doi: 10.1007/s00402-019-03127-5. Epub 2019 Feb 16.
The increasing prevalence of obesity has led to an increase in total knee arthroplasties (TKAs) being undertaken in patients with a higher body mass index (BMI). TKA in morbidly obese patients can be technically challenging due to numerous anatomical factors and patient co-morbidities. The long-term outcomes in this patient group are unclear. This systematic review aims to compare the long-term revision rates, functional outcomes and complication rates of TKAs in morbidly obese versus non-obese patients.
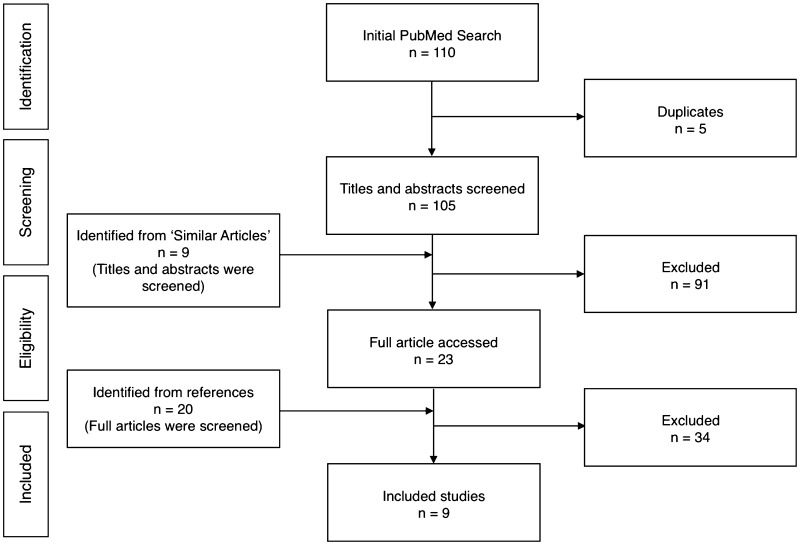
A search of PubMed, EMBASE and PubMed Central was conducted to identify studies that reported revision rates in a cohort of morbidly obese patients (BMI ≥ 40 kg/m) that underwent primary TKA, compared to non-obese patients (BMI ≤ 30 kg/m). Secondary outcomes included Knee Society Objective Scores (KSOS), Knee Society Functional Scores (KSFS), and complication rates between the two groups. The difference in revision rates was assessed using the Chi-squared test. The Wilcoxon signed-rank test was used to compare pre-operative and post-operative functional scores for each group. KSOS and KSFS for morbidly obese and non-obese patients were compared using the Mann-Whitney test. Statistical significance was defined as p ≤ 0.05.
Nine studies were included in this review. There were 624 TKAs in morbidly obese patients and 9,449 TKAs in non-obese patients, average BMI values were 45.0 kg/m (range 40-66 kg/m) and 26.5 kg/m (range 11-30 kg/m) respectively. The average follow-up time was 4.8 years (range 0.5-14.1) and 5.2 years (range 0.5-13.2) respectively, with a revision rate of 7% and 2% (p < 0.001) respectively. All functional scores improved after TKA (p < 0.001). Pre- and post-operative KSOS and KSFS were poorer in morbidly obese patients, however, mean improvement in KSOS was the same in both groups and comparable between groups for KSFS (p = 0.78). Overall complication rates, including infection, were higher in morbidly obese patients.
This review suggests an increased mid to long-term revision rate following primary TKA in morbidly obese patients, however, these patients have a functional recovery which is comparable to non-obese individuals. There is also an increased risk of perioperative complications, such as superficial wound infection. Morbidly obese patients should be fully informed of these issues prior to undergoing primary TKA.
肥胖患病率的不断上升导致体重指数(BMI)较高的患者接受全膝关节置换术(TKA)的数量增加。由于众多解剖因素和患者合并症,病态肥胖患者的TKA在技术上具有挑战性。该患者群体的长期预后尚不清楚。本系统评价旨在比较病态肥胖患者与非肥胖患者TKA的长期翻修率、功能结局和并发症发生率。
检索了PubMed、EMBASE和PubMed Central,以确定报告了一组接受初次TKA的病态肥胖患者(BMI≥40kg/m²)与非肥胖患者(BMI≤30kg/m²)翻修率的研究。次要结局包括膝关节协会客观评分(KSOS)、膝关节协会功能评分(KSFS)以及两组之间的并发症发生率。使用卡方检验评估翻修率的差异。采用Wilcoxon符号秩检验比较每组术前和术后的功能评分。使用Mann-Whitney检验比较病态肥胖患者和非肥胖患者的KSOS和KSFS。统计学显著性定义为p≤0.05。
本评价纳入了9项研究。病态肥胖患者中有624例TKA,非肥胖患者中有9449例TKA,平均BMI值分别为45.0kg/m²(范围40-66kg/m²)和26.5kg/m²(范围ll-30kg/m²)。平均随访时间分别为4.8年(范围0.5-14.1年)和5.2年(范围0.5-13.2年),翻修率分别为7%和2%(p<0.001)。TKA后所有功能评分均有所改善(p<0.001)。病态肥胖患者术前和术后的KSOS和KSFS较差,然而,两组KSOS的平均改善相同,KSFS在组间具有可比性(p=0.78)。病态肥胖患者包括感染在内的总体并发症发生率较高。
本评价表明,病态肥胖患者初次TKA后的中长期翻修率增加,然而,这些患者的功能恢复与非肥胖个体相当。围手术期并发症的风险也增加,如浅表伤口感染。在进行初次TKA之前,应将这些问题充分告知病态肥胖患者。