Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark.
Department of Primary Care and Population Health, University College London, London, United Kingdom.
PLoS One. 2019 Feb 19;14(2):e0212259. doi: 10.1371/journal.pone.0212259. eCollection 2019.
Biochemical adrenal insufficiency induced by glucocorticoid treatment is prevalent, but data on the clinical implications are sparse. We investigated clinical consequences of glucocorticoid-induced adrenal insufficiency after oral glucocorticoid cessation.
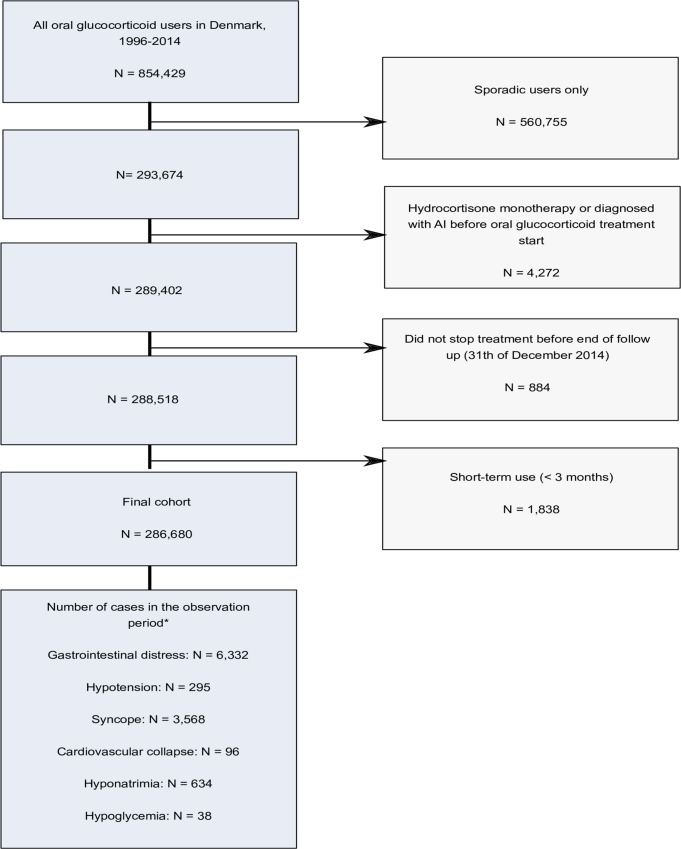
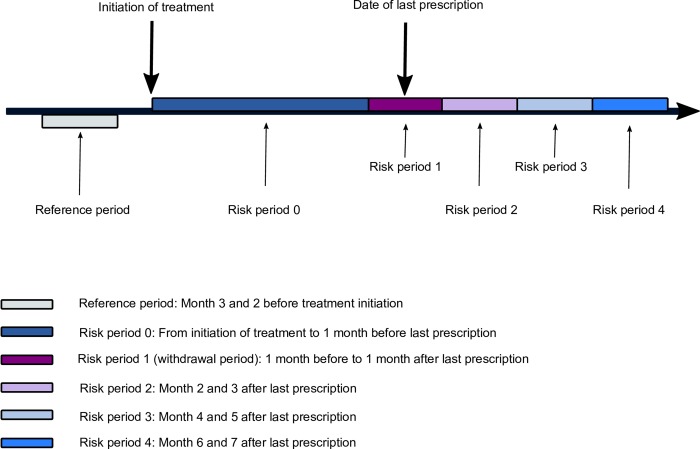
We conducted a Danish population-based self-controlled case series utilizing medical registries. In this design each individual serves as their own control allowing event rates to be compared as a function of time and treatment. Clinical indicators of adrenal insufficiency were defined as diagnoses of gastrointestinal symptoms, hypotension, cardiovascular collapse, syncope, hyponatremia, and hypoglycaemia. We included 286,680 persons who discontinued long-term (≥ 3 months) oral glucocorticoid treatment. We defined five risk periods and a reference period (before treatment): period 0 (on treatment), withdrawal period (1 month before and after cessation), followed by three consecutive 2 month-risk periods after withdrawal (periods 2-4).
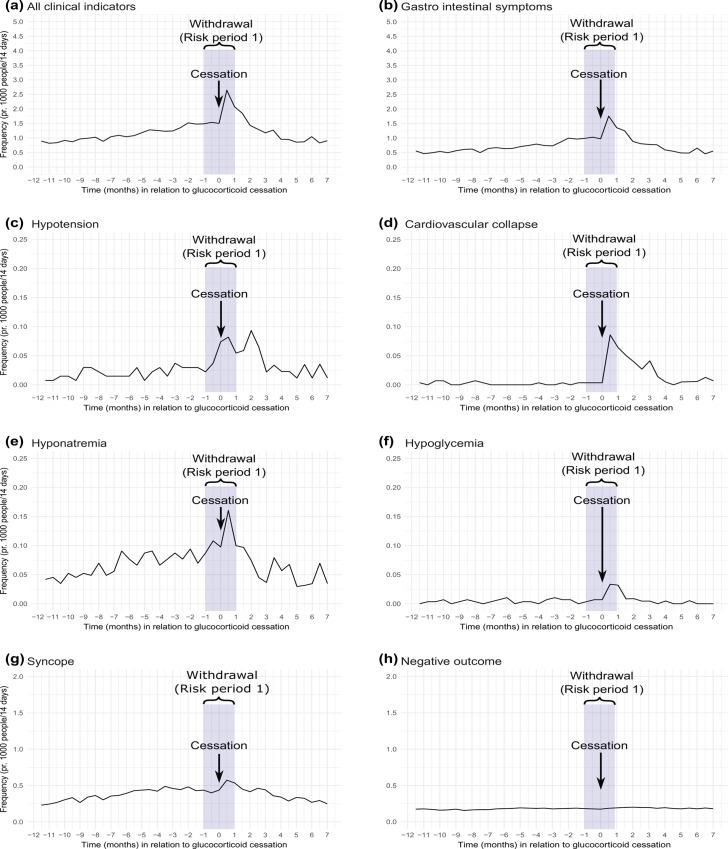
Median age at cessation was 69 years and 57% were female. Median treatment duration was 297 days and median cumulative dose was 3000 mg prednisolone equivalents. The incidence rates of hypotension, gastrointestinal symptoms, hypoglycemia and hyponatremia were increased in the withdrawal period compared to before treatment started (reference period). Incidence rate ratios comparing the withdrawal period with the reference period were 2.5 [95% confidence interval (CI): 1.4-4.3] for hypotension, 1.7 (95% CI: 1.6-1.9) for gastrointestinal symptoms, 2.2 (95% CI: 0.7-7.3) for hypoglycemia, and 1.5 (95% CI: 1.1-2.0) for hyponatremia. During 7 months of follow up, the rates of hypotension and gastrointestinal symptoms remained elevated compared to the reference period. Risk factors included use of antibiotics, increasing average daily dose of glucocorticoids, cumulative dose, and age.
Oral glucocorticoid withdrawal was associated with adverse outcomes attributable to adrenal insufficiency. Our study underscores the need for future research to establish evidence-based clinical guidance on management of patients who discontinue oral glucocorticoids.
糖皮质激素治疗引起的生化肾上腺功能不全很常见,但关于其临床意义的数据却很少。我们研究了口服糖皮质激素停药后糖皮质激素诱导的肾上腺功能不全的临床后果。
我们进行了一项基于丹麦人群的自身对照病例系列研究,利用医疗登记处进行。在这种设计中,每个人都是自己的对照,可以根据时间和治疗来比较事件发生率。肾上腺功能不全的临床指标定义为胃肠道症状、低血压、心血管衰竭、晕厥、低钠血症和低血糖的诊断。我们纳入了 286680 名停止长期(≥3 个月)口服糖皮质激素治疗的患者。我们定义了五个风险期和一个参考期(治疗前):期 0(治疗中)、停药期(停药前 1 个月和停药后),随后是停药后连续三个 2 个月的风险期(期 2-4)。
停药时的中位年龄为 69 岁,57%为女性。中位治疗持续时间为 297 天,中位累积剂量为 3000 毫克泼尼松等效物。与治疗开始前的参考期相比,停药期低血压、胃肠道症状、低血糖和低钠血症的发生率增加(参考期)。与参考期相比,比较停药期与参考期的发病率比分别为 2.5(95%置信区间:1.4-4.3)的低血压、1.7(95%置信区间:1.6-1.9)的胃肠道症状、2.2(95%置信区间:0.7-7.3)的低血糖和 1.5(95%置信区间:1.1-2.0)的低钠血症。在 7 个月的随访期间,与参考期相比,低血压和胃肠道症状的发生率仍居高不下。危险因素包括使用抗生素、糖皮质激素平均日剂量增加、累积剂量和年龄。
口服糖皮质激素停药与肾上腺功能不全引起的不良后果有关。我们的研究强调需要进一步研究,为停止口服糖皮质激素的患者制定基于证据的临床管理指南。