HIV and AIDS Malignancy Branch, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD.
Viral Oncology Section, AIDS and Cancer Virus Program, Leidos Biomedical Research, Frederick National Laboratory for Cancer Research, Frederick, MD.
Blood. 2019 Apr 18;133(16):1753-1761. doi: 10.1182/blood-2019-01-893339. Epub 2019 Feb 19.
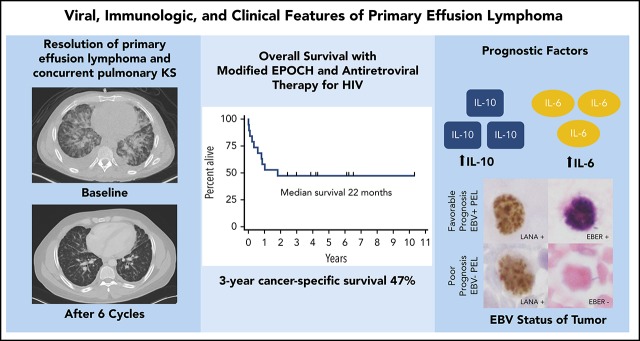
Primary effusion lymphoma (PEL) is an aggressive HIV-associated lymphoma with a relatively poor prognosis in the era of effective HIV therapy. Kaposi sarcoma herpesvirus (KSHV) is the etiologic agent, and ∼80% of tumors are coinfected with Epstein-Barr virus (EBV). A better understanding of how KSHV-related immune dysregulation contributes to the natural history of PEL will improve outcomes. Twenty patients with PEL diagnosed between 2000 and 2013, including 19 treated with modified infusional etoposide, vincristine, and doxorubicin with cyclophosphamide and prednisone (EPOCH), were identified. We compared their clinical, virologic, and immunologic features vs 20 patients with HIV-associated diffuse large B-cell lymphoma and 19 patients with symptomatic interleukin (IL)-6 related KSHV-associated multicentric Castleman disease. Survival analyses of treated patients with PEL were then performed to identify prognostic factors and cancer-specific mortality. Compared with HIV-associated diffuse large B-cell lymphoma, PEL was associated with significant hypoalbuminemia ( < .0027), thrombocytopenia ( = .0045), and elevated IL-10 levels ( < .0001). There were no significant differences in these parameters between PEL and KSHV-associated multicentric Castleman disease. Median overall survival in treated patients with PEL was 22 months, with a plateau in survival noted after 2 years. Three-year cancer-specific survival was 47%. EBV-positive tumor status was associated with improved survival (hazard ratio, 0.27; = .038), and elevated IL-6 level was associated with inferior survival (hazard ratio, 6.1; = .024). Our analysis shows that IL-6 and IL-10 levels contribute to the natural history of PEL. Inflammatory cytokines and tumor EBV status are the strongest prognostic factors. Pathogenesis-directed first-line regimens are needed to improve overall survival in PEL.
原发性渗出性淋巴瘤(PEL)是一种侵袭性的 HIV 相关淋巴瘤,在有效的 HIV 治疗时代,其预后相对较差。卡波西肉瘤疱疹病毒(KSHV)是其病原体,约 80%的肿瘤合并感染 EBV。更好地了解 KSHV 相关免疫失调如何影响 PEL 的自然史,将改善其预后。我们鉴定了 2000 年至 2013 年间诊断为 PEL 的 20 例患者,其中 19 例接受了改良的 EPOCH 方案(依托泊苷、长春新碱、多柔比星联合环磷酰胺和泼尼松)治疗。我们比较了他们的临床、病毒学和免疫学特征与 20 例 HIV 相关弥漫性大 B 细胞淋巴瘤患者和 19 例有症状的白细胞介素(IL)-6 相关 KSHV 相关多中心卡斯特曼病患者的特征。然后对接受治疗的 PEL 患者进行生存分析,以确定预后因素和癌症特异性死亡率。与 HIV 相关弥漫性大 B 细胞淋巴瘤相比,PEL 患者显著存在低白蛋白血症( <.0027)、血小板减少症( =.0045)和升高的 IL-10 水平( <.0001)。在 PEL 和 KSHV 相关多中心卡斯特曼病患者中,这些参数之间没有显著差异。接受治疗的 PEL 患者的中位总生存期为 22 个月,2 年后生存趋于平稳。3 年癌症特异性生存率为 47%。EBV 阳性肿瘤状态与生存改善相关(风险比,0.27; =.038),而升高的 IL-6 水平与生存较差相关(风险比,6.1; =.024)。我们的分析表明,IL-6 和 IL-10 水平促成了 PEL 的自然史。炎症细胞因子和肿瘤 EBV 状态是最强的预后因素。需要针对发病机制的一线方案来提高 PEL 的总生存率。