Department of Cardiology, Rigshospitalet, 2142, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark.
Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark.
ESC Heart Fail. 2019 Apr;6(2):379-387. doi: 10.1002/ehf2.12401. Epub 2019 Feb 19.
Patients with heart failure (HF) are known to have a reduced pulmonary diffusion capacity for carbon monoxide (D ), but little is known about how lung function relates to central haemodynamics. The aim of this study was to investigate the association between haemodynamic variables and pulmonary diffusion capacity adjusted for alveolar volume in congestive HF patients and to analyse how predicted D /V affects mortality in relation to the haemodynamic status.
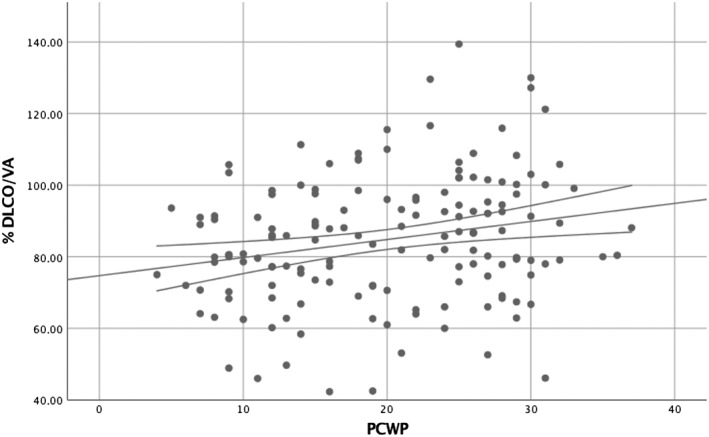
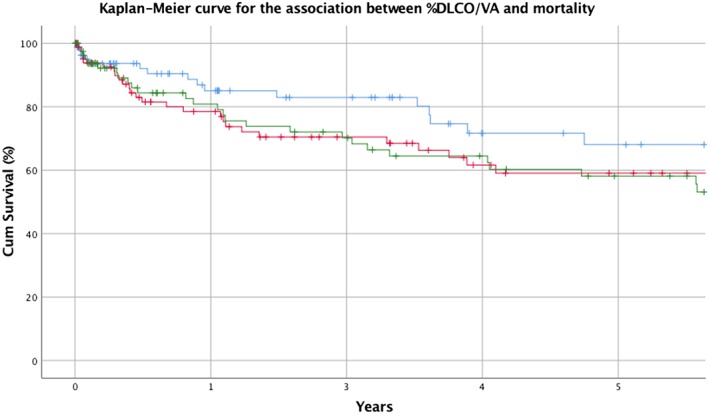
We retrospectively studied right heart catheterization (RHC) and lung function data on 262 HF patients (mean age 51 ± 13 years) with a left ventricular ejection fraction < 45% referred non-urgently for evaluation for heart transplantation (HTX) or left ventricular assist device (LVAD). Univariate and multivariate linear regression models were constructed to examine the associations between predicted values of D /V , forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV ), and haemodynamic parameters [pulmonary capillary wedge pressure (PCWP), central venous pressure, cardiac index, mean pulmonary artery pressure, and mean arterial pressure] as well as other factors known to affect lung function in HF. FEV was reduced to <80% of predicted value in 55% of the population, and D V was reduced in 63% of the population. D /V correlated positively with pulmonary capillary wedge pressure in both univariate and multivariate analyses for all included patients (P < 0.001 and P = 0.045, respectively) and a restricted population of patients with the shortest time between RHC and lung function testing (P = 0.005, P = 0.015). D /V predicted mortality in multivariate models [hazard ratio 1.5 (1.1-2.1)] but not the combined endpoint of death, LVAD implantation, or HTX. There was no significant correlation between haemodynamics and predicted FVC or FEV .
Pulmonary diffusion capacity correlates positively with left ventricular fillings pressures, and reduced values predict increased mortality in patients with HF. This might be driven by increased lung capillary volume in patients with pulmonary congestion.
已知心力衰竭(HF)患者的一氧化碳肺弥散量(D )降低,但对于肺功能与中心血液动力学的关系知之甚少。本研究旨在探讨充血性 HF 患者肺泡容积校正后的血液动力学变量与肺弥散量之间的关系,并分析预测的 D /V 如何与血液动力学状态相关影响死亡率。
我们回顾性研究了 262 例因心力衰竭(左心室射血分数<45%)而非紧急接受心脏移植(HTX)或左心室辅助装置(LVAD)评估的患者的右心导管检查(RHC)和肺功能数据。构建了单变量和多变量线性回归模型,以检查预测的 D /V 、用力肺活量(FVC)和 1 秒用力呼气量(FEV )与血液动力学参数[肺毛细血管楔压(PCWP)、中心静脉压、心指数、平均肺动脉压和平均动脉压]以及其他已知影响 HF 患者肺功能的因素之间的关系。在人群中,有 55%的患者 FEV 降低至<80%预计值,有 63%的患者 D V 降低。在所有纳入患者的单变量和多变量分析中,D /V 与肺毛细血管楔压呈正相关(均 P<0.001 和 P=0.045),并且在 RHC 和肺功能检测之间时间最短的患者的受限人群中也是如此(P=0.005,P=0.015)。D /V 在多变量模型中预测死亡率[危险比 1.5(1.1-2.1)],但不能预测 HF 患者的死亡、LVAD 植入或 HTX 的联合终点。血液动力学与预测的 FVC 或 FEV 之间无明显相关性。
肺弥散量与左心室充盈压呈正相关,降低值预示 HF 患者死亡率增加。这可能是由于肺充血患者的肺毛细血管体积增加所致。