Department of Obstetrics and Gynaecology, Amsterdam UMC, University of Amsterdam, Meibergdreef 9, 1105 AZ Amsterdam, Netherlands.
Department of Obstetrics and Gynaecology, Radboud University Medical Centre, Nijmegen, Netherlands.
BMJ. 2019 Feb 20;364:l344. doi: 10.1136/bmj.l344.
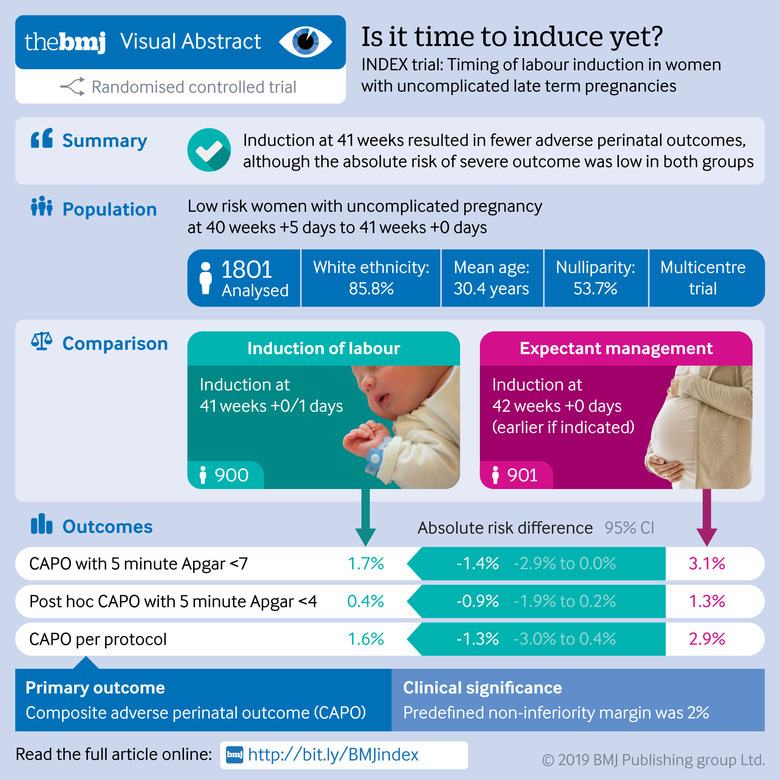
To compare induction of labour at 41 weeks with expectant management until 42 weeks in low risk women.
Open label, randomised controlled non-inferiority trial.
123 primary care midwifery practices and 45 hospitals (secondary care) in the Netherlands, 2012-16.
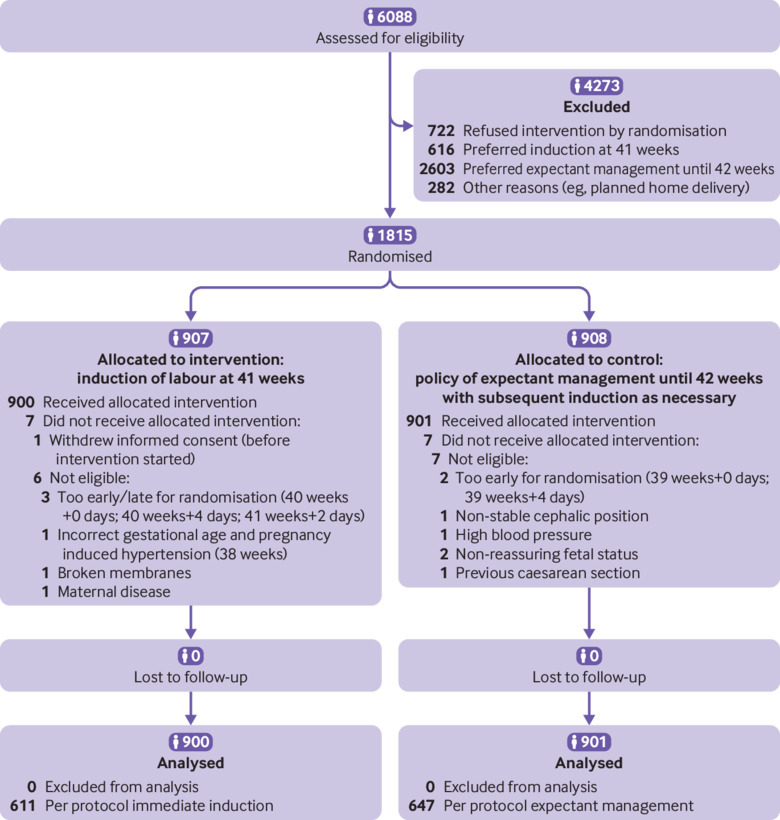
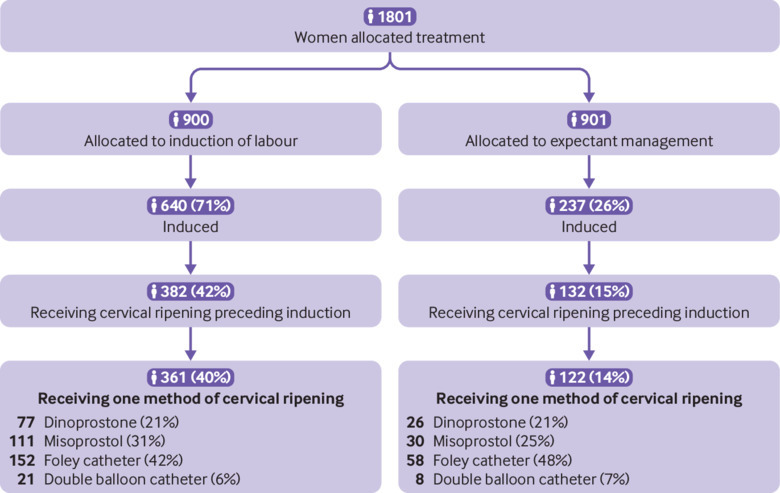
1801 low risk women with an uncomplicated singleton pregnancy: randomised to induction (n=900) or to expectant management until 42 weeks (n=901).
Induction at 41 weeks or expectant management until 42 weeks with induction if necessary.
Primary outcome was a composite of perinatal mortality and neonatal morbidity (Apgar score <7 at five minutes, arterial pH <7.05, meconium aspiration syndrome, plexus brachialis injury, intracranial haemorrhage, and admission to a neonatal intensive care unit (NICU). Secondary outcomes included maternal outcomes and mode of delivery. The null hypothesis that expectant management is inferior to induction was tested with a non-inferiority margin of 2%.
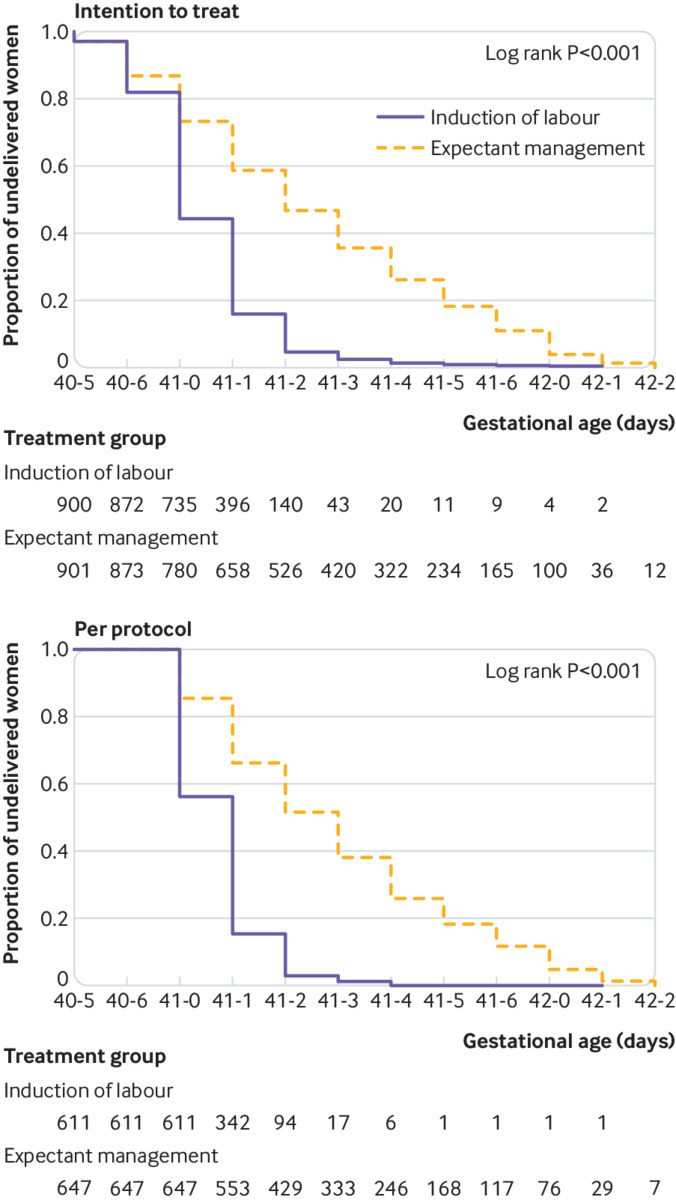
Median gestational age at delivery was 41 weeks+0 days (interquartile range 41 weeks+0 days-41 weeks+1 day) for the induction group and 41 weeks+2 days (41 weeks+0 days-41 weeks+5 days) for the expectant management group. The primary outcome was analysed for both the intention-to-treat population and the per protocol population. In the induction group, 15/900 (1.7%) women had an adverse perinatal outcome versus 28/901 (3.1%) in the expectant management group (absolute risk difference -1.4%, 95% confidence interval -2.9% to 0.0%, P=0.22 for non-inferiority). 11 (1.2%) infants in the induction group and 23 (2.6%) in the expectant management group had an Apgar score <7 at five minutes (relative risk (RR) 0.48, 95% CI 0.23 to 0.98). No infants in the induction group and three (0.3%) in the expectant management group had an Apgar score <4 at five minutes. One fetal death (0.1%) occurred in the induction group and two (0.2%) in the expectant management group. No neonatal deaths occurred. 3 (0.3%) neonates in the induction group versus 8 (0.9%) in the expectant management group were admitted to an NICU (RR 0.38, 95% CI 0.10 to 1.41). No significant difference was found in composite adverse maternal outcomes (induction n=122 (13.6%) expectant management n=102 (11.3%)) or in caesarean section rate (both groups n=97 (10.8%)).
This study could not show non-inferiority of expectant management compared with induction of labour in women with uncomplicated pregnancies at 41 weeks; instead a significant difference of 1.4% was found for risk of adverse perinatal outcomes in favour of induction, although the chances of a good perinatal outcome were high with both strategies and the incidence of perinatal mortality, Apgar score <4 at five minutes, and NICU admission low.
Netherlands Trial Register NTR3431.
比较在低危人群中,41 周时引产与 42 周时期待管理的效果。
开放标签、随机对照非劣效性试验。
荷兰 123 个基层助产士实践点和 45 家医院(二级保健),2012-2016 年。
1801 名低危、单胎妊娠、无并发症的孕妇:随机分为引产组(n=900)或期待管理组直至 42 周(n=901)。
41 周时引产或期待管理直至 42 周,必要时行引产。
主要结局为围产儿死亡率和新生儿发病率的复合指标(5 分钟时 Apgar 评分<7、动脉 pH 值<7.05、胎粪吸入综合征、臂丛神经损伤、颅内出血和新生儿重症监护病房(NICU)入院)。次要结局包括母婴结局和分娩方式。假设期待管理劣于引产的非劣效性边界为 2%。
引产组的中位分娩孕周为 41 周+0 天(四分位距 41 周+0 天-41 周+1 天),期待管理组为 41 周+2 天(41 周+0 天-41 周+5 天)。主要结局在意向治疗人群和方案人群中均进行了分析。在引产组中,15/900(1.7%)名妇女发生不良围产儿结局,而期待管理组中 28/901(3.1%)名妇女发生(绝对风险差异-1.4%,95%置信区间-2.9%至 0.0%,P=0.22 为非劣效性)。在引产组中,11(1.2%)名婴儿 5 分钟时 Apgar 评分<7,而在期待管理组中,23(2.6%)名婴儿 Apgar 评分<7(相对风险(RR)0.48,95%CI 0.23 至 0.98)。在引产组中没有婴儿 Apgar 评分<4,而在期待管理组中,有 3(0.3%)名婴儿 Apgar 评分<4。在引产组中有 1 例(0.1%)胎儿死亡,在期待管理组中有 2 例(0.2%)胎儿死亡。没有新生儿死亡。在引产组中有 3(0.3%)名新生儿入住 NICU,而在期待管理组中有 8(0.9%)名新生儿入住 NICU(RR 0.38,95%CI 0.10 至 1.41)。在复合不良母婴结局(引产组 n=122(13.6%),期待管理组 n=102(11.3%))或剖宫产率(两组均 n=97(10.8%))方面,未发现显著差异。
本研究未能显示在 41 周时,期待管理与引产相比在无并发症的妊娠中不具有非劣效性;相反,引产的围产儿不良结局风险显著增加 1.4%,尽管两种策略的围产儿结局良好的可能性都很高,且围产儿死亡率、5 分钟时 Apgar 评分<4 和 NICU 入院率都较低。
荷兰临床试验注册处 NTR3431。