Department of Molecular and Clinical Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, 416 85, Gothenburg, Sweden.
Department of Cardiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Clin Res Cardiol. 2019 Sep;108(9):1025-1033. doi: 10.1007/s00392-019-01430-0. Epub 2019 Feb 20.
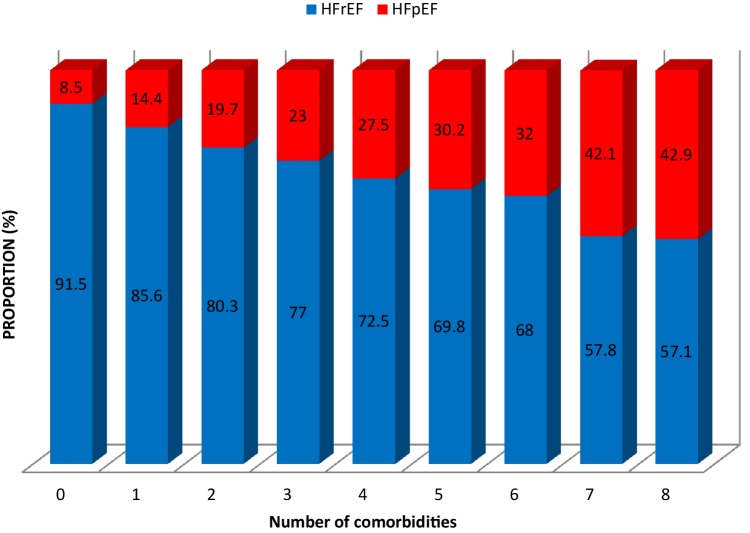
Heart failure (HF) and non-cardiac comorbidities often coexist and are known to have an adverse effect on outcome. However, the prevalence and prognostic impact of non-cardiac comorbidities in patients with HF with reduced ejection fraction (HFrEF) vs. those with preserved (HFpEF) remain inadequately studied.
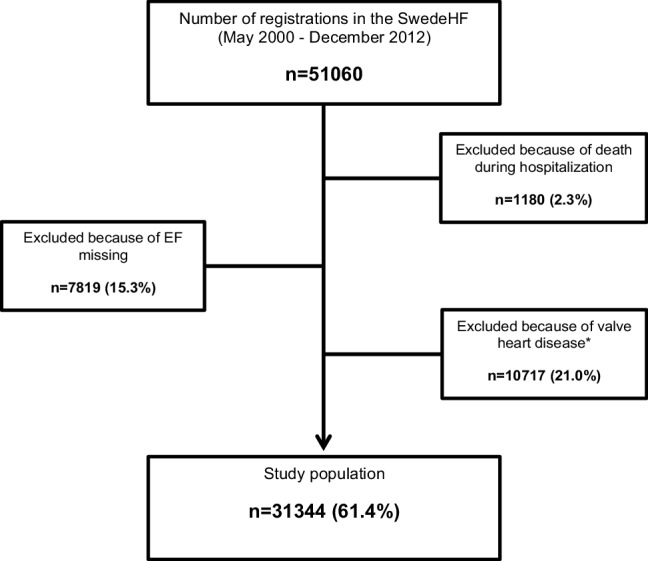
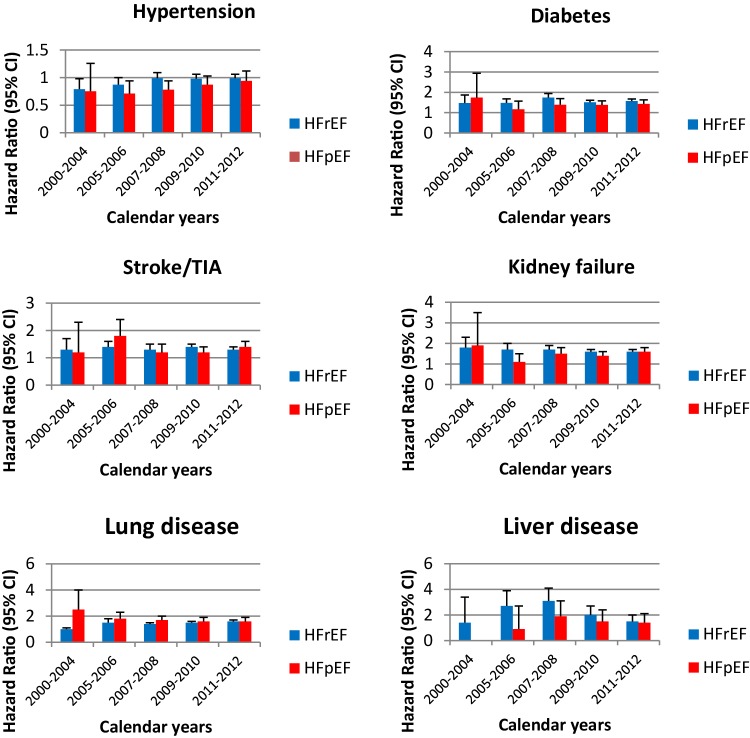
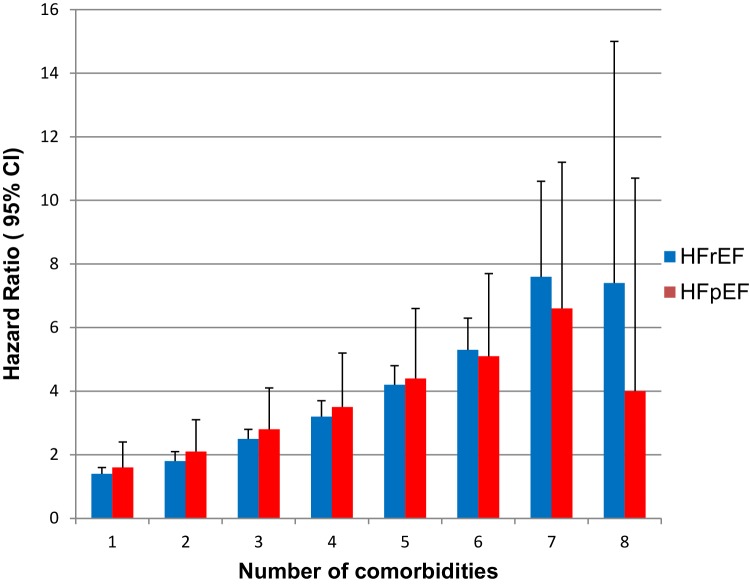
We used data from the Swedish Heart Failure Registry from 2000 to 2012. HFrEF was defined as EF < 50% and HFpEF as EF ≥ 50%. Of 31 344 patients available for analysis, 79.3% (n = 24 856) had HFrEF and 20.7% (n = 6 488) HFpEF. The outcome was all-cause mortality. We examined the association between ten non-cardiac comorbidities and mortality and its interaction with EF using adjusted hazard ratio (HR). Stroke, anemia, gout and cancer had a similar impact on mortality in both phenotypes, whereas diabetes (HR 1.57, 95% confidence interval [CI] [1.50-1.65] vs. HR 1.39 95% CI [1.27-1.51], p = 0.0002), renal failure (HR 1.65, 95% CI [1.57-1.73] vs. HR 1.44, 95% CI [1.32-1.57], p = 0.003) and liver disease (HR 2.13, 95% CI [1.83-2.47] vs. HR 1.42, 95% CI [1.09-1.85] p = 0.02) had a higher impact in the HFrEF patients. Moreover, pulmonary disease (HR 1.46, 95% CI [1.40-1.53] vs. HR 1.66 95% CI [1.54-1.80], p = 0.007) was more prominent in the HFpEF patients. Sleep apnea was not associated with worse prognosis in either group. No significant variation was found in the impact over the 12-year study period.
Non-cardiac comorbidities contribute significantly but differently to mortality, both in HFrEF and HFpEF. No significant variation was found in the impact over the 12-year study period. These results emphasize the importance of including the management of comorbidities as a part of a standardized heart failure care in both HF phenotypes.
心力衰竭(HF)和非心脏合并症常同时存在,并已知对预后有不良影响。然而,射血分数降低的心力衰竭(HFrEF)与射血分数保留的心力衰竭(HFpEF)患者中非心脏合并症的患病率和预后影响仍研究不足。
我们使用了 2000 年至 2012 年瑞典心力衰竭注册处的数据。HFrEF 的定义为 EF<50%,HFpEF 的定义为 EF≥50%。在可分析的 31344 例患者中,79.3%(n=24856)为 HFrEF,20.7%(n=6488)为 HFpEF。结局为全因死亡率。我们使用调整后的危险比(HR)检查了十种非心脏合并症与死亡率之间的关系及其与 EF 的相互作用。卒中、贫血、痛风和癌症在两种表型中对死亡率的影响相似,而糖尿病(HR 1.57,95%置信区间[CI] [1.50-1.65] vs. HR 1.39,95%CI [1.27-1.51],p=0.0002)、肾功能衰竭(HR 1.65,95%CI [1.57-1.73] vs. HR 1.44,95%CI [1.32-1.57],p=0.003)和肝病(HR 2.13,95%CI [1.83-2.47] vs. HR 1.42,95%CI [1.09-1.85],p=0.02)在 HFrEF 患者中的影响更高。此外,在 HFpEF 患者中,肺部疾病(HR 1.46,95%CI [1.40-1.53] vs. HR 1.66,95%CI [1.54-1.80],p=0.007)更为突出。在这两个组中,睡眠呼吸暂停与预后不良均无显著相关性。在 12 年的研究期间,未发现影响有显著变化。
非心脏合并症对 HFrEF 和 HFpEF 患者的死亡率均有显著但不同的影响。在 12 年的研究期间,未发现影响有显著变化。这些结果强调了在两种心力衰竭表型中,将合并症的管理作为标准化心力衰竭治疗的一部分的重要性。