Department of Surgery, Cancer Centre Amsterdam, Amsterdam UMC, Vrije Universiteit Amsterdam, De Boelelaan, 1117, Amsterdam, The Netherlands.
Department of Radiology & Nuclear Medicine, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands.
Eur J Nucl Med Mol Imaging. 2019 Jul;46(7):1495-1505. doi: 10.1007/s00259-019-04284-w. Epub 2019 Feb 23.
Using current optical imaging techniques and gamma imaging modalities, perioperative sentinel lymph node (SLN) identification in colon cancer can be difficult when the SLN is located near the primary tumour or beneath a thick layer of (fat) tissue. Sentinel lymph node mapping using PET/CT lymphoscintigraphy combined with real-time visualization of the SLN using near-infrared imaging has shown promising results in several types of cancer and may facilitate the successful identification of the number and location of the SLN in early colon cancer.
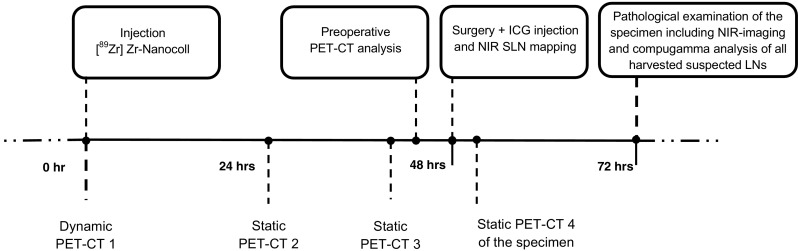
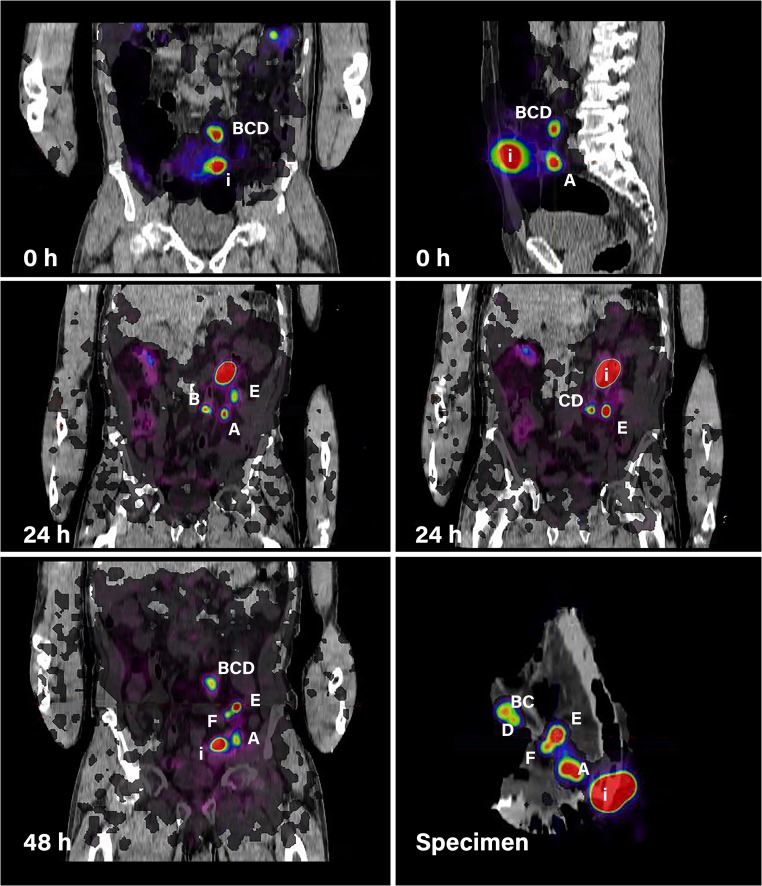
Clinical feasibility of PET/CT lymphoscintigraphy using preoperative endoscopically injected [Zr]Zr-Nanocoll and intraoperative injection of the near-infrared (NIR) tracer Indocyanine Green (ICG) was evaluated in ten early colon cancer patients. Three preoperative PET/CT scans and an additional ex vivo scan of the specimen were performed after submucosal injection of [Zr]Zr-Nanocoll. All SLNs and other lymph nodes underwent extensive pathological examination for metastases. A histopathological proven lymph node visible at preoperative PET/CT and identified at PET/CT of the specimen was defined as SLN.
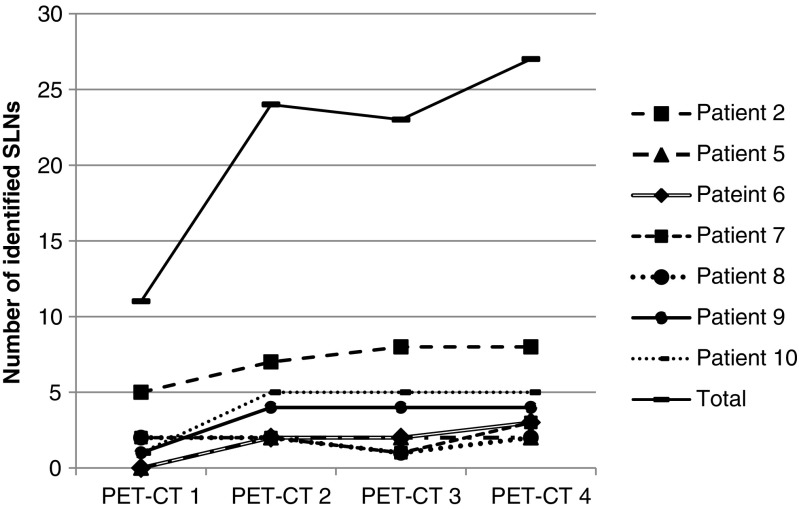
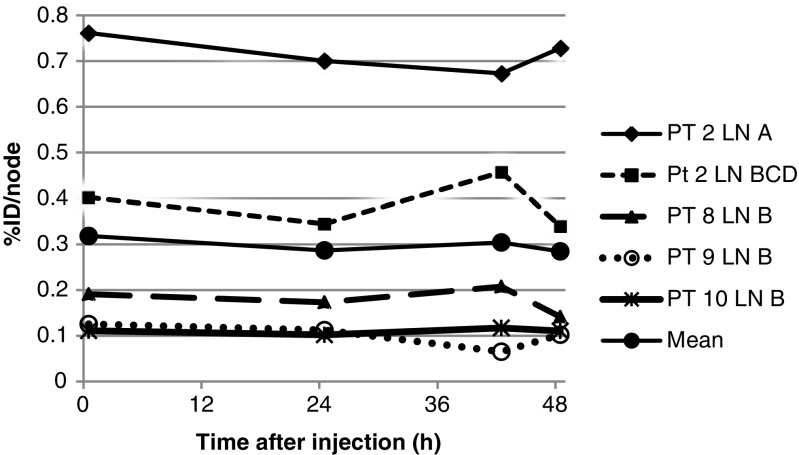
A total of 27 SLNs were harvested in seven out of eight patients with successful injection of both tracers. In one patient no SLNs were assigned preoperatively. In two patients injection of [Zr]Zr-Nanocoll failed due to incorrect needle positioning. Twenty-one (78%) SLNs were found intraoperatively using NIR-imaging. Eleven of the 27 (41%) SLNs were located near the primary tumour (< 2 cm). Those six SLNs not found intraoperatively with NIR-imaging were all located close to the tumour. In all seven patients at least one SLN could be assigned at preoperative imaging 24 h after tracer administration. One SLN contained metastases detected by immunohistochemistry. No metastases were found in the non-SLNs.
This study shows the potential of preoperative PET/CT lymphoscintigraphy to inform the surgeon about the number and location of SLNs in patients with early colon cancer. The additional use of NIR-imaging allows for intraoperative identification of these SLNs which are invisible with conventional white light imaging. Further research is necessary to improve and simplify the technique. We recommend perioperative SLN identification using a preoperative lymphoscintigraphy scan just before surgery approximately 24 h after injection. Additionally a postoperative scan of the specimen combined with intraoperative real-time NIR-imaging should be performed.
在 SLN 位于原发肿瘤附近或厚层(脂肪)组织下方时,使用当前的光学成像技术和伽马成像方式,对结肠癌进行围手术期前哨淋巴结 (SLN) 识别较为困难。使用 PET/CT 淋巴闪烁显像术结合 SLN 近红外成像的实时可视化进行 SLN 定位,已在多种癌症中显示出良好的效果,并可能有助于成功识别早期结肠癌中 SLN 的数量和位置。
对 10 例早期结肠癌患者进行了术前经内镜注射 [Zr]Zr-Nanocoll 和术中注射近红外(NIR)示踪剂吲哚菁绿(ICG)的 PET/CT 淋巴闪烁显像术的临床可行性评估。在黏膜下注射 [Zr]Zr-Nanocoll 后,进行了 3 次术前 PET/CT 扫描和对标本的额外离体扫描。所有 SLN 和其他淋巴结均进行了广泛的转移病理学检查。在术前 PET/CT 上可见并在标本的 PET/CT 上识别的经组织病理学证实的淋巴结被定义为 SLN。
在 8 例成功注射两种示踪剂的患者中,共检出 27 个 SLN,其中 7 例检出。在 1 例患者中,术前未分配 SLN。由于不正确的针头定位,有 2 例患者未能注射 [Zr]Zr-Nanocoll。使用 NIR 成像技术,21 个(78%)SLN 术中被发现。27 个 SLN 中的 11 个(41%)位于原发肿瘤附近(<2cm)。那些术中未用 NIR 成像找到的 6 个 SLN 均靠近肿瘤。在所有 7 例患者中,在示踪剂给药后 24 小时进行术前成像,至少可以在术前成像中分配一个 SLN。1 个 SLN 含有免疫组化检测到的转移。非 SLN 中未发现转移。
本研究表明,术前 PET/CT 淋巴闪烁显像术有潜力告知外科医生早期结肠癌患者 SLN 的数量和位置。额外使用 NIR 成像可识别术中用常规白光成像无法识别的这些 SLN。有必要进一步研究以改进和简化该技术。我们建议在术前淋巴结闪烁显像术扫描前约 24 小时,即在手术前进行围手术期前哨淋巴结识别,并在术后对标本进行扫描,并结合术中实时 NIR 成像。