Department of Surgery, Cancer Center Amsterdam, Amsterdam UMC-Vrije Universiteit Amsterdam, De Boelelaan 1117, Amsterdam, The Netherlands.
Department of Operating Rooms and MITeC Technology Center, Radboud University Medical Center, Nijmegen, The Netherlands.
Tech Coloproctol. 2019 Dec;23(12):1113-1126. doi: 10.1007/s10151-019-02107-6. Epub 2019 Nov 18.
Near-infrared (NIR) fluorescence imaging has the potential to overcome the current drawbacks of sentinel lymph node mapping (SLNM) in colon cancer. Our aim was to provide an overview of current SLNM performance and of factors influencing successful sentinel lymph node (SLN) identification using NIR fluorescence imaging in colon cancer.
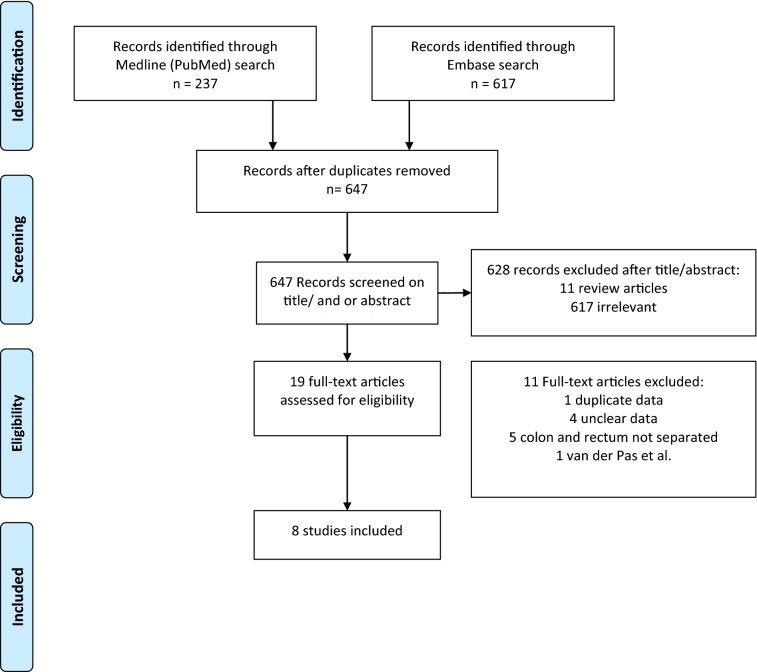
A systematic review and meta-analysis was conducted to identify currently used methods and results. Additionally, we performed a single-center study using indocyanine green (ICG) as SLNM dye in colon cancer patients scheduled for a laparoscopic colectomy. SLNs were analyzed with conventional hematoxylin-and-eosin staining and additionally with serial sectioning and immunohistochemistry (extended histopathological assessment). A true-positive procedure was defined as a tumor-positive SLN either by conventional hematoxylin-and-eosin staining or by extended histopathological assessment, independently of regional lymph node status. SLN procedures were determined to be true negatives if SLNs and regional lymph nodes revealed no metastases after conventional and advanced histopathology. SLN procedures yielding tumor-negative SLNs in combination with tumor-positive regional lymph nodes were classified as false negatives. Sensitivity, negative predictive value and detection rate were calculated.
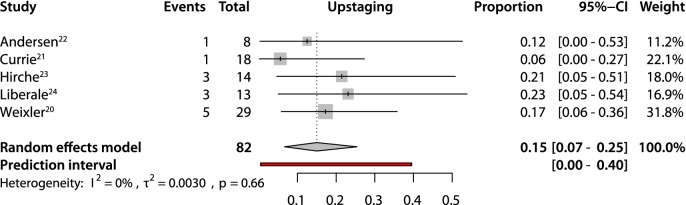
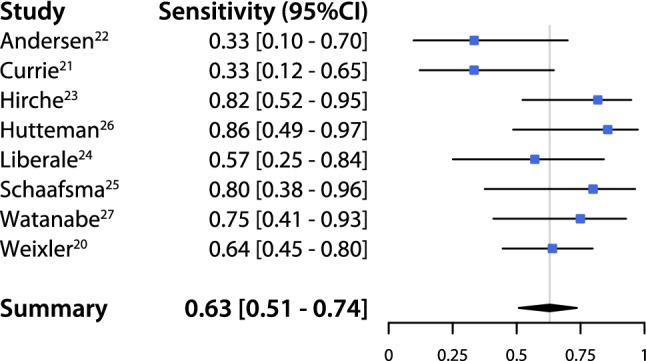
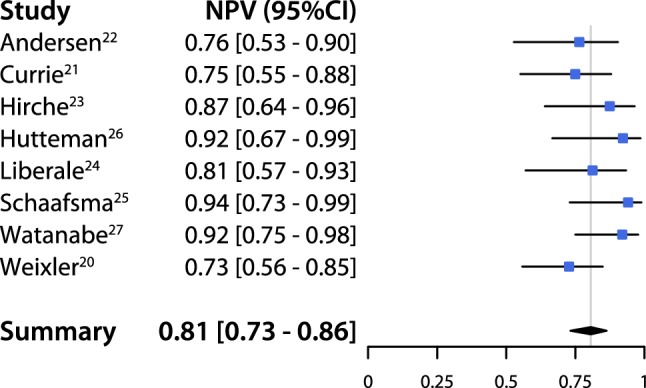
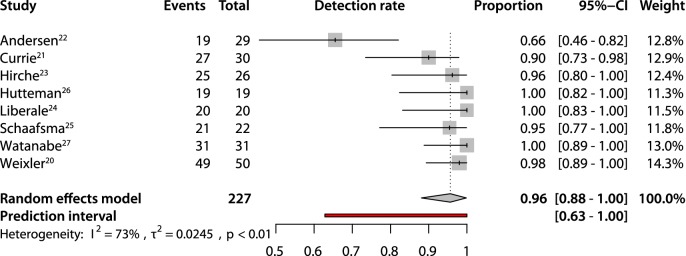
This systematic review and meta-analysis included 8 studies describing 227 SLN procedures. A pooled sensitivity of 0.63 (95% CI 0.51-0.74), negative predictive value 0.81 (95% CI 0.73-0.86) and detection rate of 0.94 (95% CI 0.85-0.97) were found. Upstaging as a result of extended histopathological assessment was 0.15 (95% CI 0.07-0.25). In our single-center study, we included 30 patients. Five false-negative SLNs were identified, resulting in a sensitivity of 44% and negative predictive value of 80%, with a detection rate of 89.7%. Eight patients had lymph node metastases, in three cases detected after extended pathological assessment, resulting in an upstaging of 13% (3 of 23 patients with negative nodes by conventional hematoxylin and eosin staining).
Several anatomical and technical difficulties make SLNM with NIR fluorescence imaging in colon cancer particularly challenging when compared to other types of cancer. As a consequence, reports of SLNM accuracy vary widely. Future studies should try to standardize the SLNM procedure and focus on early-stage colon tumors, validation of tracer composition, injection mode and improvement of real-time optical guidance.
近红外(NIR)荧光成像是克服当前结直肠癌前哨淋巴结(SLN)定位的局限性的一种潜在方法。我们的目的是提供结直肠癌中使用 NIR 荧光成像进行 SLN 识别的当前性能概述以及影响成功识别前哨淋巴结(SLN)的因素。
系统回顾和荟萃分析用于确定当前使用的方法和结果。此外,我们在计划接受腹腔镜结肠切除术的结直肠癌患者中使用吲哚菁绿(ICG)作为 SLNM 染料进行了单中心研究。使用常规苏木精-伊红(H&E)染色以及连续切片和免疫组织化学(扩展的组织病理学评估)分析 SLN。真正的阳性程序定义为通过常规苏木精-伊红染色或通过扩展的组织病理学评估检测到的肿瘤阳性 SLN,独立于区域淋巴结状态。如果 SLN 和区域淋巴结在常规和先进的组织病理学检查后均未发现转移,则将 SLN 程序确定为真正的阴性。将产生肿瘤阴性 SLN 且同时伴有肿瘤阳性区域淋巴结的 SLN 程序分类为假阴性。计算了敏感性、阴性预测值和检出率。
本系统回顾和荟萃分析包括 8 项描述 227 例 SLN 程序的研究。发现合并敏感性为 0.63(95%CI 0.51-0.74),阴性预测值为 0.81(95%CI 0.73-0.86),检出率为 0.94(95%CI 0.85-0.97)。扩展的组织病理学评估导致的升级为 0.15(95%CI 0.07-0.25)。在我们的单中心研究中,我们纳入了 30 例患者。发现 5 例假阴性 SLN,敏感性为 44%,阴性预测值为 80%,检出率为 89.7%。8 例患者存在淋巴结转移,其中 3 例在经过扩展的病理评估后发现,导致升级为 13%(3 例常规苏木精和伊红染色阴性的患者中有 23 例)。
与其他类型的癌症相比,结直肠癌中使用 NIR 荧光成像进行 SLNM 时存在多种解剖和技术上的困难,因此 SLNM 准确性的报告差异很大。未来的研究应尝试标准化 SLNM 程序,重点关注早期结直肠肿瘤、示踪剂成分的验证、注射方式以及实时光学引导的改进。