Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, London, UK.
School of Population Health and Environmental Sciences, Faculty of Life Sciences and Medicine, King's College London, London, UK.
Med Decis Making. 2019 Jan;39(1):21-31. doi: 10.1177/0272989X18813357.
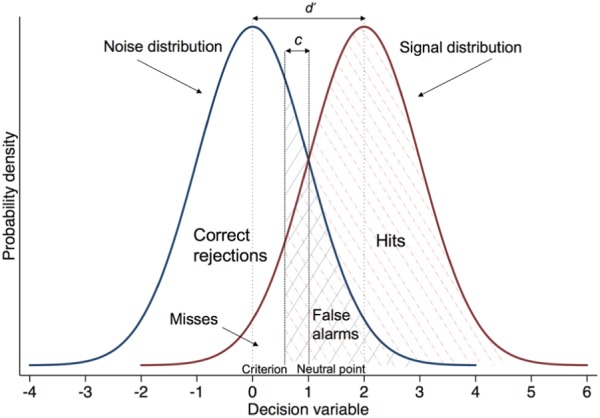
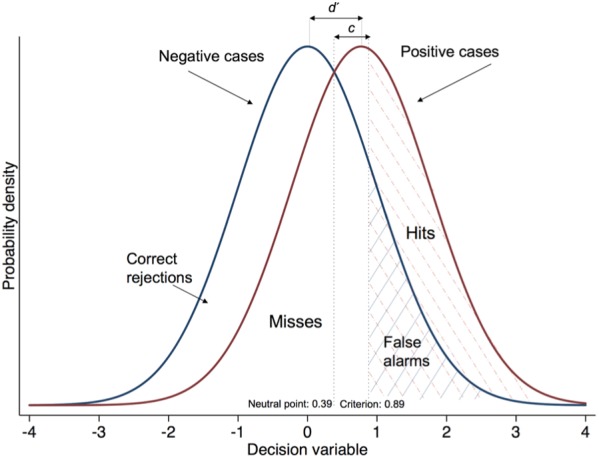
Signal detection theory (SDT) describes how respondents categorize ambiguous stimuli over repeated trials. It measures separately "discrimination" (ability to recognize a signal amid noise) and "criterion" (inclination to respond "signal" v. "noise"). This is important because respondents may produce the same accuracy rate for different reasons. We employed SDT to measure the referral decision making of general practitioners (GPs) in cases of possible lung cancer.
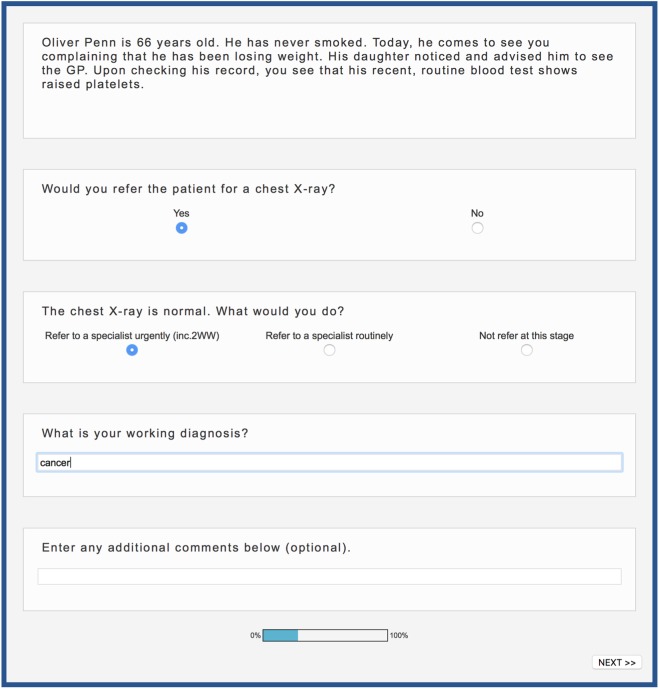
We constructed 44 vignettes of patients for whom lung cancer could be considered and estimated their 1-year risk. Under UK risk-based guidelines, half of the vignettes required urgent referral. We recruited 216 GPs from practices across England. Practices differed in the positive predictive value (PPV) of their urgent referrals (chance of referrals identifying cancer) and the sensitivity (chance of cancer patients being picked up via urgent referral from their practice). Participants saw the vignettes online and indicated whether they would refer each patient urgently or not. We calculated each GP's discrimination ( d ') and criterion ( c) and regressed these on practice PPV and sensitivity, as well as on GP experience and gender.
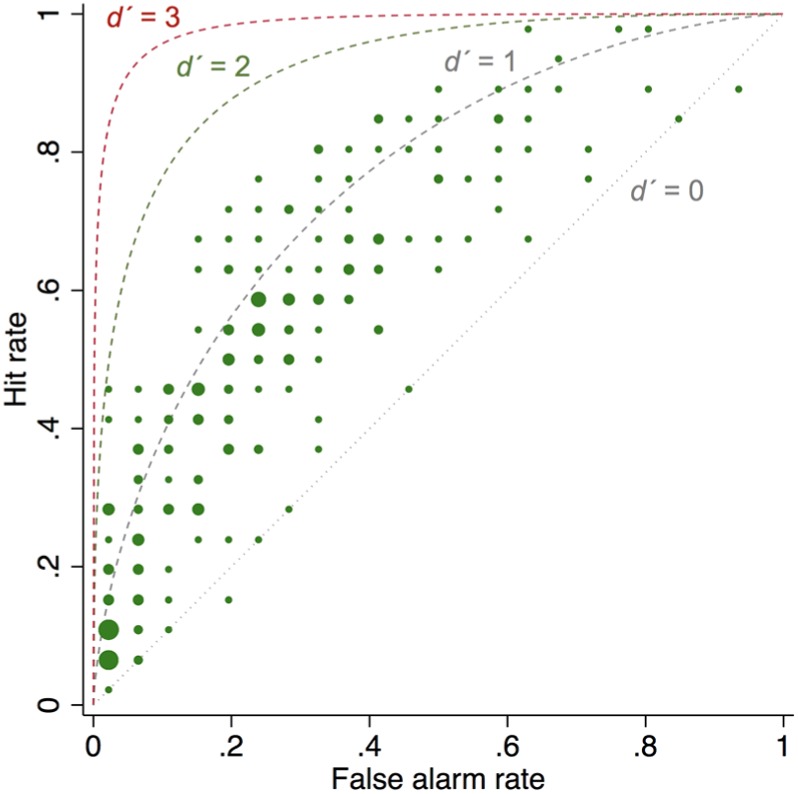
Criterion was associated with practice PPV: as PPV increased, GPs' c also increased, indicating lower inclination to refer ( b = 0.06 [0.02-0.09]; P = 0.001). Female GPs were more inclined to refer than male GPs ( b = -0.20 [-0.40 to -0.001]; P = 0.049). Average discrimination was modest ( d' = 0.77), highly variable (range, -0.28 to 1.91), and not associated with practice referral performance.
High referral PPV at the organizational level indicates GPs' inclination to avoid false positives, not better discrimination. Rather than bluntly mandating increases in practice PPV via more referrals, it is necessary to increase discrimination by improving the evidence base for cancer referral decisions.
信号检测理论(SDT)描述了被试者在重复试验中如何对模棱两可的刺激进行分类。它分别测量“辨别力”(在噪声中识别信号的能力)和“判别标准”(倾向于回应“信号”而非“噪声”)。这很重要,因为被试者可能会因为不同的原因产生相同的准确率。我们采用 SDT 来衡量全科医生(GP)在疑似肺癌病例中的转诊决策。
我们构建了 44 个可能患有肺癌的患者病例,并估计了他们的 1 年风险。根据英国基于风险的指南,这些病例中有一半需要紧急转诊。我们从英格兰各地的实践中招募了 216 名全科医生。实践中紧急转诊的阳性预测值(PPV,即转诊识别癌症的机会)和敏感性(通过实践中的紧急转诊识别癌症患者的机会)有所不同。参与者在线查看病例并表明他们是否会紧急转诊每个患者。我们计算了每位 GP 的辨别力(d')和判别标准(c),并将这些值与实践中的 PPV 和敏感性以及 GP 经验和性别进行回归分析。
判别标准与实践中的 PPV 相关:随着 PPV 的增加,GP 的 c 也随之增加,表明他们更倾向于不转诊(b=0.06[0.02-0.09];P=0.001)。女性 GP 比男性 GP 更倾向于转诊(b=-0.20[-0.40 至-0.001];P=0.049)。平均辨别力适中(d'=0.77),高度可变(范围为-0.28 至 1.91),与实践转诊表现无关。
组织层面上高的转诊 PPV 表明 GP 倾向于避免假阳性,而不是更好的辨别力。与其通过增加转诊来简单地强制提高实践中的 PPV,不如通过提高癌症转诊决策的证据基础来提高辨别力。