Program in Genetics and Genome Biology, The Hospital for Sick Children, Toronto, ON, Canada.
Department of Statistical Sciences, University of Toronto, Toronto, ON, Canada.
PLoS Genet. 2019 Feb 26;15(2):e1008007. doi: 10.1371/journal.pgen.1008007. eCollection 2019 Feb.
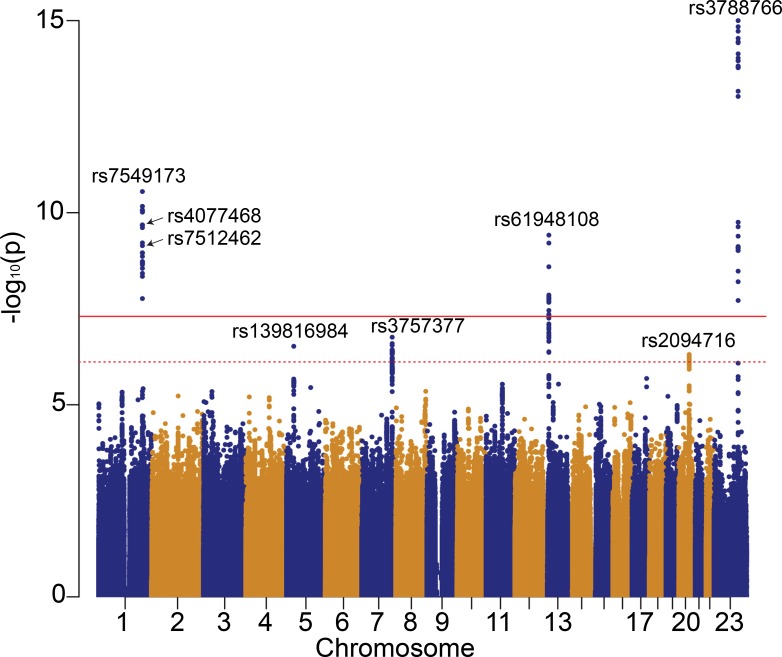
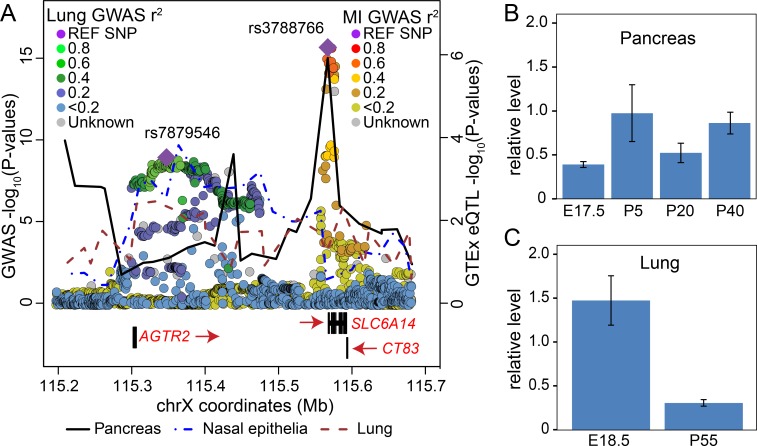
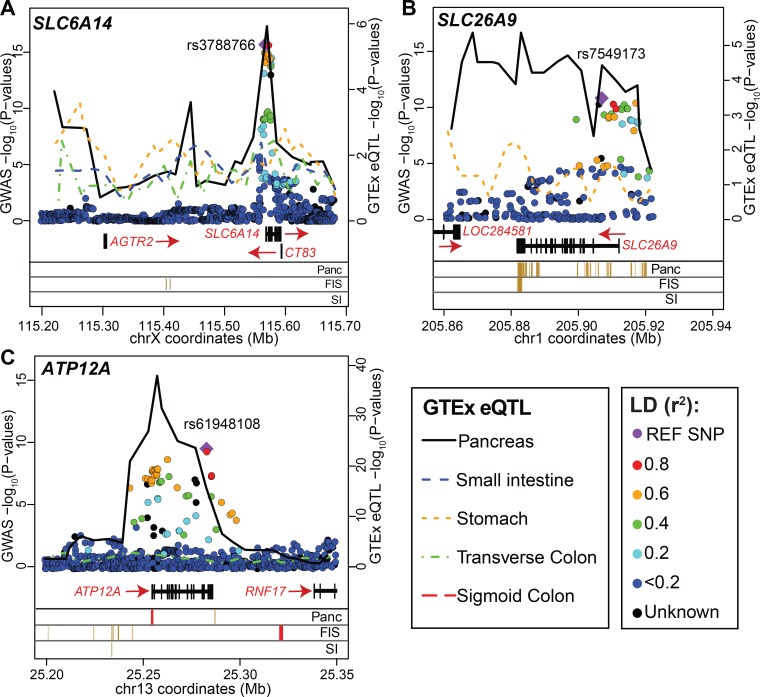
Cystic Fibrosis (CF) exhibits morbidity in several organs, including progressive lung disease in all patients and intestinal obstruction at birth (meconium ileus) in ~15%. Individuals with the same causal CFTR mutations show variable disease presentation which is partly attributed to modifier genes. With >6,500 participants from the International CF Gene Modifier Consortium, genome-wide association investigation identified a new modifier locus for meconium ileus encompassing ATP12A on chromosome 13 (min p = 3.83x10(-10)); replicated loci encompassing SLC6A14 on chromosome X and SLC26A9 on chromosome 1, (min p<2.2x10(-16), 2.81x10(-11), respectively); and replicated a suggestive locus on chromosome 7 near PRSS1 (min p = 2.55x10(-7)). PRSS1 is exclusively expressed in the exocrine pancreas and was previously associated with non-CF pancreatitis with functional characterization demonstrating impact on PRSS1 gene expression. We thus asked whether the other meconium ileus modifier loci impact gene expression and in which organ. We developed and applied a colocalization framework called the Simple Sum (SS) that integrates regulatory and genetic association information, and also contrasts colocalization evidence across tissues or genes. The associated modifier loci colocalized with expression quantitative trait loci (eQTLs) for ATP12A (p = 3.35x10(-8)), SLC6A14 (p = 1.12x10(-10)) and SLC26A9 (p = 4.48x10(-5)) in the pancreas, even though meconium ileus manifests in the intestine. The meconium ileus susceptibility locus on chromosome X appeared shifted in location from a previously identified locus for CF lung disease severity. Using the SS we integrated the lung disease association locus with eQTLs from nasal epithelia of 63 CF participants and demonstrated evidence of colocalization with airway-specific regulation of SLC6A14 (p = 2.3x10(-4)). Cystic Fibrosis is realizing the promise of personalized medicine, and identification of the contributing organ and understanding of tissue specificity for a gene modifier is essential for the next phase of personalizing therapeutic strategies.
囊性纤维化 (CF) 在多个器官中表现出病态,包括所有患者的肺部进行性疾病和约 15%的患者出生时的肠梗阻(胎粪性肠梗阻)。具有相同因果 CFTR 突变的个体表现出不同的疾病表现,部分归因于修饰基因。通过来自国际 CF 基因修饰物联合会的 6500 多名参与者,全基因组关联研究确定了一个新的胎粪性肠梗阻修饰基因座,涵盖染色体 13 上的 ATP12A(最小 p = 3.83x10(-10));复制的基因座包括染色体 X 上的 SLC6A14 和染色体 1 上的 SLC26A9(最小 p<2.2x10(-16)、2.81x10(-11));以及染色体 7 上靠近 PRSS1 的提示性基因座(最小 p = 2.55x10(-7))。PRSS1 仅在外分泌胰腺中表达,先前与非 CF 胰腺炎相关,功能特征表明其对 PRSS1 基因表达的影响。因此,我们询问其他胎粪性肠梗阻修饰基因座是否影响基因表达以及在哪个器官。我们开发并应用了一种称为简单和 (SS) 的共定位框架,该框架集成了调节和遗传关联信息,并且还比较了组织或基因之间的共定位证据。相关修饰基因座与胰腺中的 ATP12A(p = 3.35x10(-8))、SLC6A14(p = 1.12x10(-10))和 SLC26A9(p = 4.48x10(-5))的表达数量性状基因座 (eQTL) 共定位,尽管胎粪性肠梗阻表现为肠道疾病。染色体 X 上的胎粪性肠梗阻易感性基因座似乎从先前确定的 CF 肺部疾病严重程度的基因座发生了位置偏移。使用 SS,我们将肺部疾病关联基因座与 63 名 CF 参与者的鼻上皮中的 eQTL 整合在一起,并证明了 SLC6A14 的气道特异性调节的共定位证据(p = 2.3x10(-4))。囊性纤维化正在实现个性化医疗的承诺,确定基因修饰物的贡献器官和理解组织特异性对于下一阶段的个性化治疗策略至关重要。