1Intensive Care Unit, IIS La FE, Hospital Universitario y Politécnico La Fe, Valencia, Spain.
2Microbiology Department, Hospital Universitario y Politécnico La Fe, Valencia, Spain.
Antimicrob Resist Infect Control. 2019 Feb 14;8:38. doi: 10.1186/s13756-019-0484-8. eCollection 2019.
The aim of this study is to evaluate the risk factors for colonisation by multidrug resistant (MDR) in a critical care unit and the relationship between colonisation and the antibiotic pressure exerted by the antimicrobial treatments received by patients.
A prospective observational was designed. Patients admitted for more than 48 h to an intensive care unit were included. Samples for surveillance cultures were obtained from all the patients upon admission and once a week. The association between risk factors and colonisation by MDR was determined by logistic regression. A Cox regression model was used to evaluate the effect of the use of antimicrobials on the colonisation rate. An ARMIA model was used to investigate the association between the incidence of colonisation by MDR strains and the global consumption of antimicrobials in the unit.
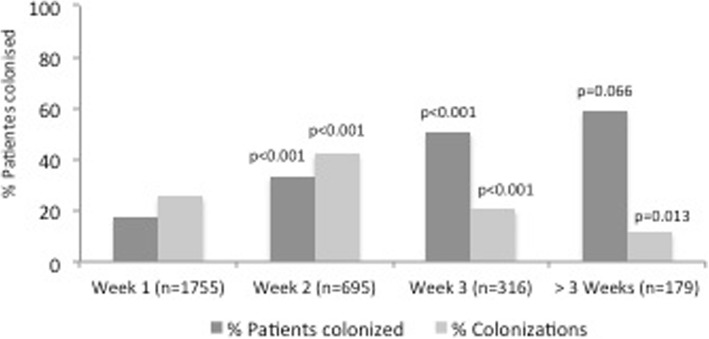
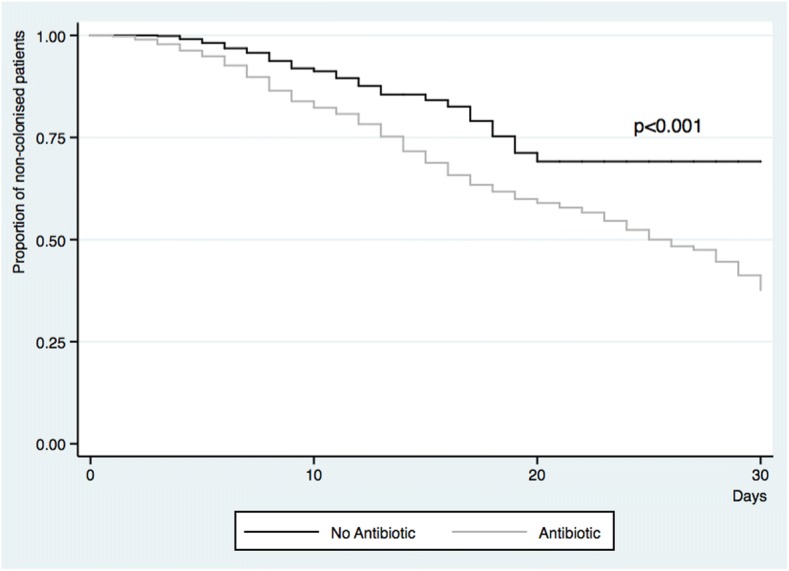
One thousand seven hundred twenty-five patients were included, from which 308 (17.9%) were positive for MDR . In the multivariate analysis, hospitalisation for longer than 7 days together with respiratory infection and administration of any antibiotic was associated with increased MR colonisation. Patients who received antibiotics for more than 48 h were colonised earlier than patients who did not receive antibiotic treatment [HR: 2.16 (95%CI:1.55-3.03)]. The ARIMA model found a significant association between the monthly colonisation rate for MR and the consumption of cephalosporins and carbapenems in the previous month.
Individual antibiotic administration and the global antibiotic pressure of cephalosporins and carbapenems are associated to an increased colonisation by MDR strains.
本研究旨在评估重症监护病房(ICU)中多重耐药菌(MDR)定植的危险因素,以及定植与患者接受的抗菌治疗所施加的抗生素压力之间的关系。
设计了一项前瞻性观察性研究。纳入 ICU 住院时间超过 48 小时的患者。所有患者入院时和每周一次采集监测培养样本。通过逻辑回归确定危险因素与 MDR 定植之间的关系。使用 Cox 回归模型评估抗菌药物使用对定植率的影响。使用 ARMIA 模型研究 MDR 定植的发生率与单位内抗菌药物总消耗量之间的关系。
共纳入 1725 例患者,其中 308 例(17.9%)为 MDR 定植阳性。多变量分析显示,住院时间超过 7 天、呼吸道感染和使用任何抗生素与 MR 定植增加相关。接受抗生素治疗超过 48 小时的患者比未接受抗生素治疗的患者更早定植[HR:2.16(95%CI:1.55-3.03)]。ARIMA 模型发现 MR 每月定植率与前一个月头孢菌素和碳青霉烯类抗生素消耗之间存在显著关联。
个体抗生素的使用和头孢菌素及碳青霉烯类抗生素的整体抗生素压力与 MDR 定植的增加有关。