1 Department of Cardiology Asklepios Klinik St. Georg Hamburg Germany.
2 Department of Cardiology University Heart Center Zurich Switzerland.
J Am Heart Assoc. 2019 Mar 5;8(5):e010365. doi: 10.1161/JAHA.118.010365.
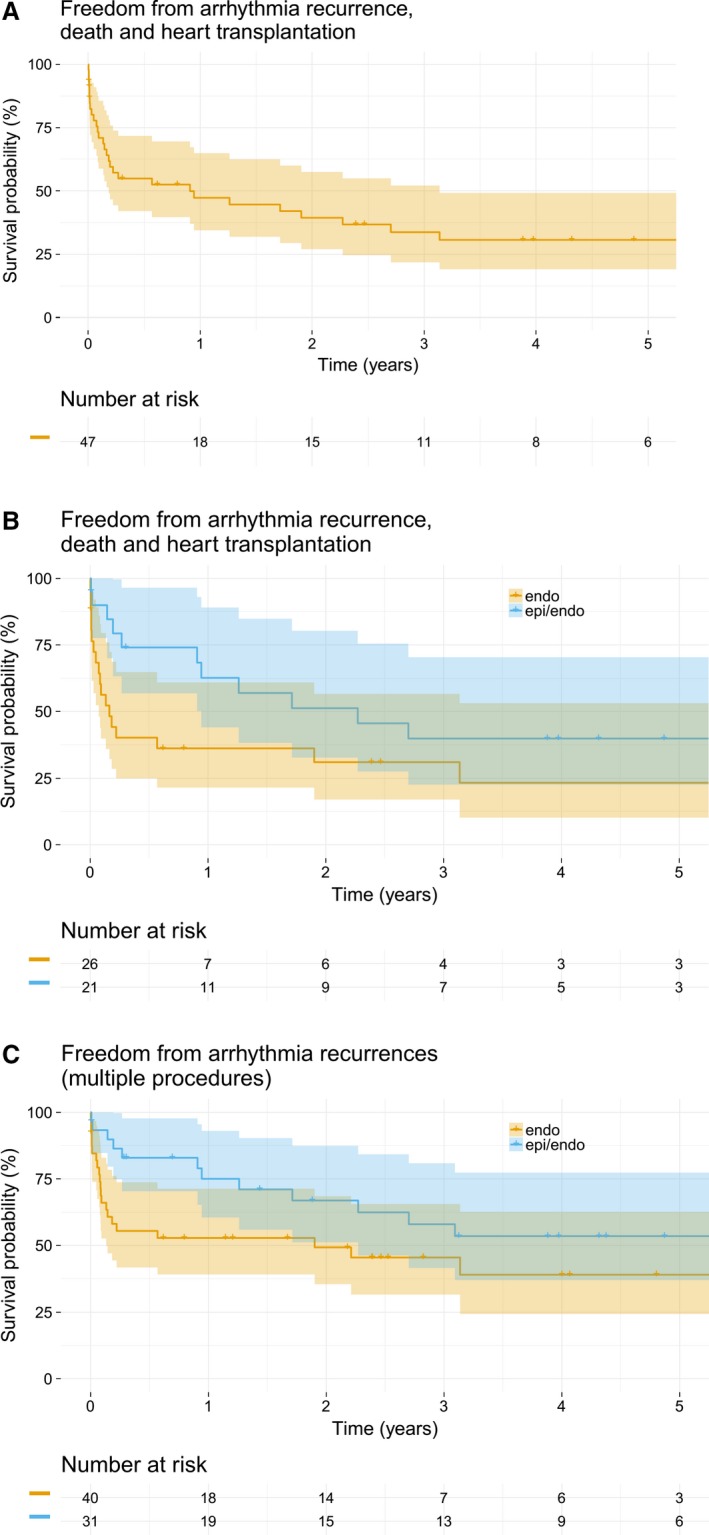
Background It has been suggested that endocardial and epicardial ablation of ventricular tachycardia ( VT ) improves outcome in arrhythmogenic right ventricular cardiomyopathy/dysplasia. We investigated our sequential approach for VT ablation in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia in a single center. Methods and Results We included 47 patients (44±16 years) with definite (81%) or borderline (19%) arrhythmogenic right ventricular cardiomyopathy/dysplasia between 1998 and 2016. Our ablation strategy was to target the endocardial substrate. Epicardial ablation was performed in case of acute ablation failure or lack of an endocardial substrate. Single and multiple procedural 1- and 5-year outcome data for the first occurrence of the study end points (sustained VT /ventricular fibrillation, heart transplant, and death after the index procedure, and sustained VT /ventricular fibrillation for multiple procedures) are reported. Eighty-one radiofrequency ablation procedures were performed (mean 1.7 per patient, range 1-4). Forty-five (56%) ablation procedures were performed via an endocardial, 11 (13%) via an epicardial, and 25 (31%) via a combined endo- and epicardial approach. Complete acute success was achieved in 65 (80%) procedures, and partial success in 13 (16%). After a median follow-up of 50.8 (interquartile range, [18.6; 99.2]) months after the index procedure, 17 (36%) patients were free from the primary end point. After multiple procedures, freedom from sustained VT /ventricular fibrillation was 63% (95% CI , 52-75) at 1 year, and 45% (95% CI , 34-61) at 5 years, with 36% of patients receiving only endocardial radiofrequency ablation. A trend (log rank P=0.058) towards an improved outcome using a combined endo-/epicardial approach was observed after multiple procedures. Conclusion Endocardial ablation can be effective in a considerable number of arrhythmogenic right ventricular cardiomyopathy/dysplasia patients with VT , potentially obviating the need for an epicardial approach.
已有研究表明,对室性心动过速(VT)进行心内膜和心外膜消融可改善心律失常性右室心肌病/发育不良患者的预后。我们在单一中心研究了我们对心律失常性右室心肌病/发育不良患者 VT 消融的序贯方法。
我们纳入了 1998 年至 2016 年间明确(81%)或边界(19%)心律失常性右室心肌病/发育不良的 47 例患者(44±16 岁)。我们的消融策略是靶向心内膜基质。如果急性消融失败或不存在心内膜基质,则进行心外膜消融。报告了首次出现研究终点(持续性 VT/室颤、心脏移植和指数手术后死亡,以及多次程序的持续性 VT/室颤)的单程序和多程序 1 年和 5 年的结果数据。共进行了 81 次射频消融术(平均每位患者 1.7 次,范围 1-4 次)。45 次(56%)消融术通过心内膜进行,11 次(13%)通过心外膜进行,25 次(31%)通过心内-心外膜联合进行。65 次(80%)手术即刻完全成功,13 次(16%)部分成功。在指数手术后中位随访 50.8(四分位距 [18.6;99.2])个月后,17 例(36%)患者无主要终点事件。多次手术后,1 年时持续性 VT/室颤无复发率为 63%(95%CI,52-75),5 年时为 45%(95%CI,34-61),其中 36%的患者仅接受心内膜射频消融。多次手术后,联合心内-心外膜方法的结局呈改善趋势(对数秩 P=0.058)。
在心内膜消融术能有效治疗相当一部分心律失常性右室心肌病/发育不良伴 VT 的患者,可能避免心外膜方法的应用。