Yale School of Public Health, PO Box 208034, New Haven, CT, 06520-8034, USA.
Medical Practice Evaluation Center, Massachusetts General Hospital, Harvard Medical School, 100 Cambridge Street, Boston, MA, 02114, USA.
BMC Public Health. 2019 Feb 27;19(1):236. doi: 10.1186/s12889-019-6533-7.
Area-level deprivation is associated with multiple adverse birth outcomes. Few studies have examined the mediating pathways through which area-level deprivation affects these outcomes. The objective of this study was to investigate the association between area-level deprivation and preterm birth, and examine the mediating effects of maternal medical, behavioural, and psychosocial factors.
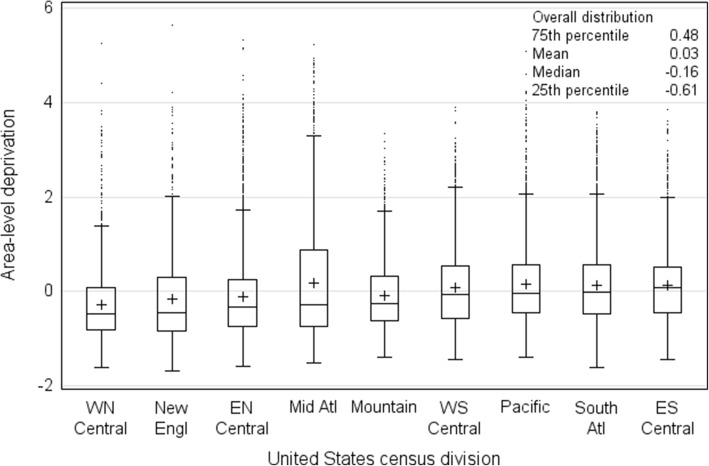
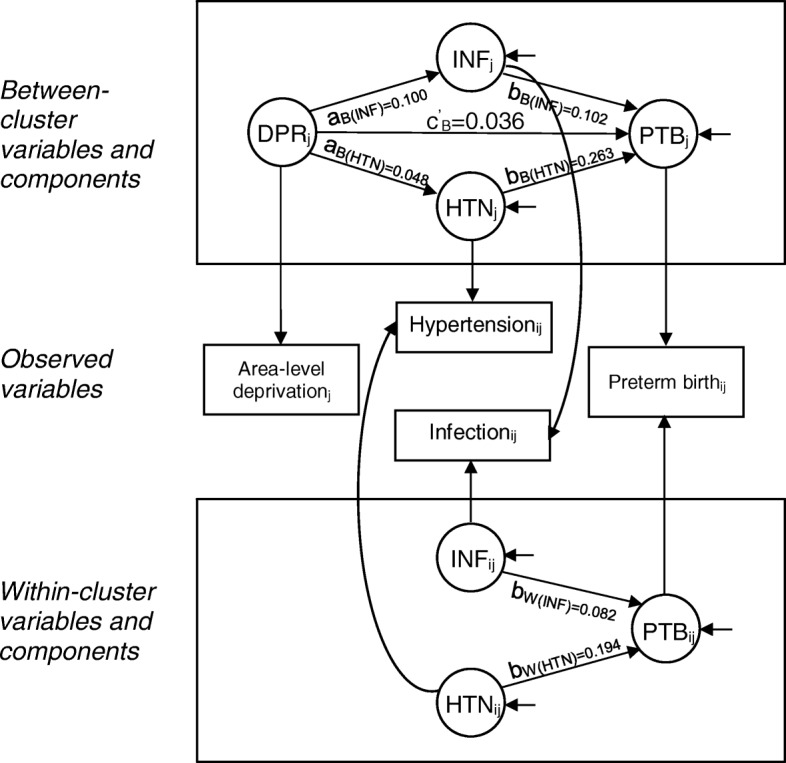
We conducted a retrospective cohort study using national, commercial health insurance claims data from 2011, obtained from the Health Care Cost Institute. Area-level deprivation was derived from principal components methods using ZIP code-level data. Multilevel structural equation modeling was used to examine mediating effects.
In total, 138,487 women with a live singleton birth residing in 14,577 ZIP codes throughout the United States were included. Overall, 5.7% of women had a preterm birth. In fully adjusted generalized estimation equation models, compared to women in the lowest quartile of area-level deprivation, odds of preterm birth increased by 9.6% among women in the second highest quartile (odds ratio (OR) 1.096; 95% confidence interval (CI) 1.021, 1.176), by 11.3% in the third highest quartile (OR 1.113; 95% CI 1.035, 1.195), and by 24.9% in the highest quartile (OR 1.249; 95% CI 1.165, 1.339). Hypertension and infection moderately mediated this association.
Even among commercially-insured women, area-level deprivation was associated with increased risk of preterm birth. Similar to individual socioeconomic status, area-level deprivation does not have a threshold effect. Implementation of policies to reduce area-level deprivation, and the screening and treatment of maternal mediators may be associated with a lower risk of preterm birth.
区域贫困与多种不良出生结局相关。很少有研究探讨区域贫困影响这些结局的中介途径。本研究旨在调查区域贫困与早产之间的关联,并检验产妇医疗、行为和心理社会因素的中介作用。
我们使用来自健康成本研究所的 2011 年全国商业健康保险索赔数据进行了回顾性队列研究。区域贫困程度是通过使用邮政编码级别的数据进行主成分方法得出的。采用多层次结构方程模型检验中介效应。
共纳入了 138487 名居住在美国 14577 个邮政编码区域的单胎活产妇女。总体而言,有 5.7%的妇女早产。在完全调整的广义估计方程模型中,与处于区域贫困程度最低四分位数的妇女相比,处于第二高四分位数的妇女早产的几率增加了 9.6%(比值比 1.096;95%置信区间 1.021,1.176),处于第三高四分位数的妇女增加了 11.3%(比值比 1.113;95%置信区间 1.035,1.195),处于最高四分位数的妇女增加了 24.9%(比值比 1.249;95%置信区间 1.165,1.339)。高血压和感染在一定程度上介导了这种关联。
即使在商业保险的妇女中,区域贫困与早产风险增加相关。与个体社会经济地位相似,区域贫困没有阈值效应。实施减少区域贫困的政策,以及对产妇中介因素的筛查和治疗,可能与较低的早产风险相关。