Royal College of Obstetricians and Gynaecologists, London, United Kingdom; Department of Health Services Research, Faculty of Public Health and Policy, London School of Hygiene and Tropical Medicine, London, United Kingdom.
Royal College of Obstetricians and Gynaecologists, London, United Kingdom.
Am J Obstet Gynecol. 2021 Nov;225(5):522.e1-522.e11. doi: 10.1016/j.ajog.2021.05.016. Epub 2021 May 20.
Some studies have suggested that women with SARS-CoV-2 infection during pregnancy are at increased risk of adverse pregnancy and neonatal outcomes, but these associations are still not clear.
This study aimed to determine the association between SARS-CoV-2 infection at the time of birth and maternal and perinatal outcomes.
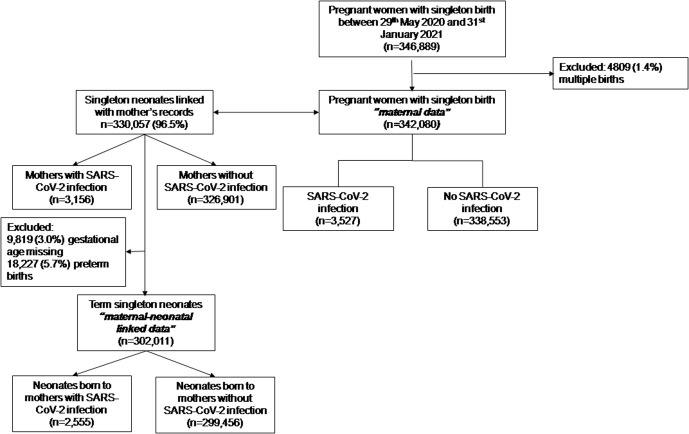
This is a population-based cohort study in England. The inclusion criteria were women with a recorded singleton birth between May 29, 2020, and January 31, 2021, in a national database of hospital admissions. Maternal and perinatal outcomes were compared between pregnant women with a laboratory-confirmed SARS-CoV-2 infection recorded in the birth episode and those without. Study outcomes were fetal death at or beyond 24 weeks' gestation (stillbirth), preterm birth (<37 weeks' gestation), small for gestational age infant (small for gestational age; birthweight at the <tenth centile), preeclampsia or eclampsia, induction of labor, mode of birth, specialist neonatal care, composite neonatal adverse outcome indicator, maternal and neonatal length of hospital stay after birth (3 days or more), and 28-day neonatal and 42-day maternal hospital readmission. Adjusted odds ratios and their 95% confidence interval for the association between SARS-CoV-2 infection status and outcomes were calculated using logistic regression, adjusting for maternal age, ethnicity, parity, preexisting diabetes mellitus, preexisting hypertension, and socioeconomic deprivation measured using the Index of Multiple Deprivation 2019. Models were fitted with robust standard errors to account for hospital-level clustering. The analysis of the neonatal outcomes was repeated for those born at term (≥37 weeks' gestation) because preterm birth has been reported to be more common in pregnant women with SARS-CoV-2 infection.
The analysis included 342,080 women, of whom 3527 had laboratory-confirmed SARS-CoV-2 infection. Laboratory-confirmed SARS-CoV-2 infection was more common in women who were younger, of non-White ethnicity, primiparous, or residing in the most deprived areas or had comorbidities. Fetal death (adjusted odds ratio, 2.21; 95% confidence interval, 1.58-3.11; P<.001) and preterm birth (adjusted odds ratio, 2.17; 95% confidence interval, 1.96-2.42; P<.001) occurred more frequently in women with SARS-CoV-2 infection than those without. The risk of preeclampsia or eclampsia (adjusted odds ratio, 1.55; 95% confidence interval, 1.29-1.85; P<.001), birth by emergency cesarean delivery (adjusted odds ratio, 1.63; 95% confidence interval, 1.51-1.76; P<.001), and prolonged admission after birth (adjusted odds ratio, 1.57; 95% confidence interval, 1.44-1.72; P<.001) were significantly higher for women with SARS-CoV-2 infection than those without. There were no significant differences (P>.05) in the rate of other maternal outcomes. The risk of neonatal adverse outcome (adjusted odds ratio, 1.45; 95% confidence interval, 1.27-1.66; P<.001), need for specialist neonatal care (adjusted odds ratio, 1.24; 95% confidence interval, 1.02-1.51; P=.03), and prolonged neonatal admission after birth (adjusted odds ratio, 1.61; 95% confidence interval, 1.49-1.75; P<.001) were all significantly higher for infants with mothers with laboratory-confirmed SARS-CoV-2 infection. When the analysis was restricted to pregnancies delivered at term (≥37 weeks), there were no significant differences in neonatal adverse outcome (P=.78), need for specialist neonatal care after birth (P=.22), or neonatal readmission within 4 weeks of birth (P=.05). Neonates born at term to mothers with laboratory-confirmed SARS-CoV-2 infection were more likely to have prolonged admission after birth (21.1% compared with 14.6%; adjusted odds ratio, 1.61; 95% confidence interval, 1.49-1.75; P<.001).
SARS-CoV-2 infection at the time of birth is associated with higher rates of fetal death, preterm birth, preeclampsia, and emergency cesarean delivery. There were no additional adverse neonatal outcomes, other than those related to preterm delivery. Pregnant women should be counseled regarding risks of SARS-CoV-2 infection and should be considered a priority for vaccination.
一些研究表明,在妊娠期间感染 SARS-CoV-2 的女性发生不良妊娠和新生儿结局的风险增加,但这些关联仍不清楚。
本研究旨在确定 SARS-CoV-2 在出生时感染与产妇和围产期结局之间的关系。
这是一项在英格兰进行的基于人群的队列研究。纳入标准为在全国住院数据库中记录的 5 月 29 日至 2021 年 1 月 31 日之间记录的单胎分娩的女性。比较在分娩时记录的实验室确诊的 SARS-CoV-2 感染的孕妇与未感染的孕妇的产妇和围产期结局。研究结局为妊娠 24 周及以上(死胎)、早产(<37 周)、小于胎龄儿(小于胎龄儿;出生体重处于第 10 百分位数以下)、子痫前期或子痫、引产、分娩方式、专科新生儿护理、复合新生儿不良结局指标、产后住院(3 天或以上)、新生儿和产妇 28 天和 42 天的住院时间,以及新生儿和产妇 28 天和 42 天的住院时间。使用逻辑回归计算 SARS-CoV-2 感染状态与结局之间的关联的调整优势比及其 95%置信区间,调整因素包括母亲年龄、种族、产次、既往糖尿病、既往高血压和 2019 年多因素剥夺指数测量的社会经济剥夺程度。为了考虑到医院层面的聚类,使用稳健标准误差拟合模型。由于在 SARS-CoV-2 感染的孕妇中,早产更为常见,因此对足月(≥37 周)出生的新生儿结局进行了重复分析。
分析纳入了 342080 名女性,其中 3527 名实验室确诊为 SARS-CoV-2 感染。与未感染的女性相比,年轻、非白人、初产妇、居住在最贫困地区或合并有合并症的女性,实验室确诊的 SARS-CoV-2 感染更为常见。SARS-CoV-2 感染的女性中,胎儿死亡(调整优势比,2.21;95%置信区间,1.58-3.11;P<.001)和早产(调整优势比,2.17;95%置信区间,1.96-2.42;P<.001)的发生率高于未感染的女性。子痫前期或子痫(调整优势比,1.55;95%置信区间,1.29-1.85;P<.001)、紧急剖宫产分娩(调整优势比,1.63;95%置信区间,1.51-1.76;P<.001)和产后住院时间延长(调整优势比,1.57;95%置信区间,1.44-1.72;P<.001)的风险也显著高于未感染的女性。与未感染的女性相比,感染的女性在其他产妇结局方面没有显著差异(P>.05)。新生儿不良结局(调整优势比,1.45;95%置信区间,1.27-1.66;P<.001)、需要专科新生儿护理(调整优势比,1.24;95%置信区间,1.02-1.51;P=.03)和产后新生儿住院时间延长(调整优势比,1.61;95%置信区间,1.49-1.75;P<.001)的风险均显著升高。患有 SARS-CoV-2 感染母亲的婴儿的这些不良新生儿结局的发生率也显著升高。当分析仅限于足月(≥37 周)分娩的妊娠时,新生儿不良结局(P=.78)、出生后需要专科新生儿护理(P=.22)或出生后 4 周内新生儿再入院(P=.05)均无显著差异。实验室确诊为 SARS-CoV-2 感染的母亲所生的足月新生儿,其住院时间延长的可能性更大(21.1%比 14.6%;调整优势比,1.61;95%置信区间,1.49-1.75;P<.001)。
出生时 SARS-CoV-2 感染与胎儿死亡、早产、子痫前期和紧急剖宫产分娩的发生率较高相关。除了与早产有关的不良新生儿结局外,没有其他不良新生儿结局。应向孕妇提供 SARS-CoV-2 感染的风险咨询,并应将其视为接种疫苗的优先事项。