Burns Michael, Singh Anurag K, Hoefer Carrie C, Zhang Yali, Wallace Paul K, Chen George L, Platek Alexis, Winslow Timothy B, Iovoli Austin J, Choi Christopher, Ross Maureen, McCarthy Philip L, Hahn Theresa
Department of Medicine, Roswell Park Comprehensive Cancer Center, Buffalo, NY 14263, United States.
Department of Radiation Medicine, Roswell Park Comprehensive Cancer Center, Buffalo, NY 14263, United States.
World J Clin Oncol. 2019 Feb 24;10(2):86-97. doi: 10.5306/wjco.v10.i2.86.
To investigate infused hematopoietic cell doses and their interaction with conditioning regimen intensity +/- total body irradiation (TBI) on outcomes after peripheral blood hematopoietic cell transplant (PBHCT).
Our retrospective cohort included 247 patients receiving a first, T-replete, human leukocyte antigen-matched allogeneic PBHCT and treated between 2001 and 2012. Correlations were calculated using the Pearson product-moment correlation coefficient. Overall survival and progression free survival curves were generated using the Kaplan-Meier method and compared using the log-rank test.
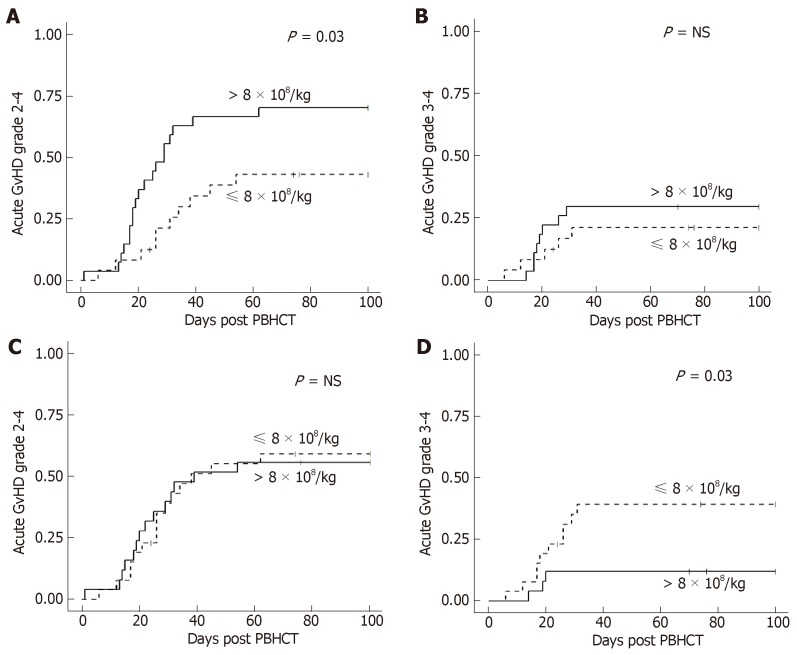
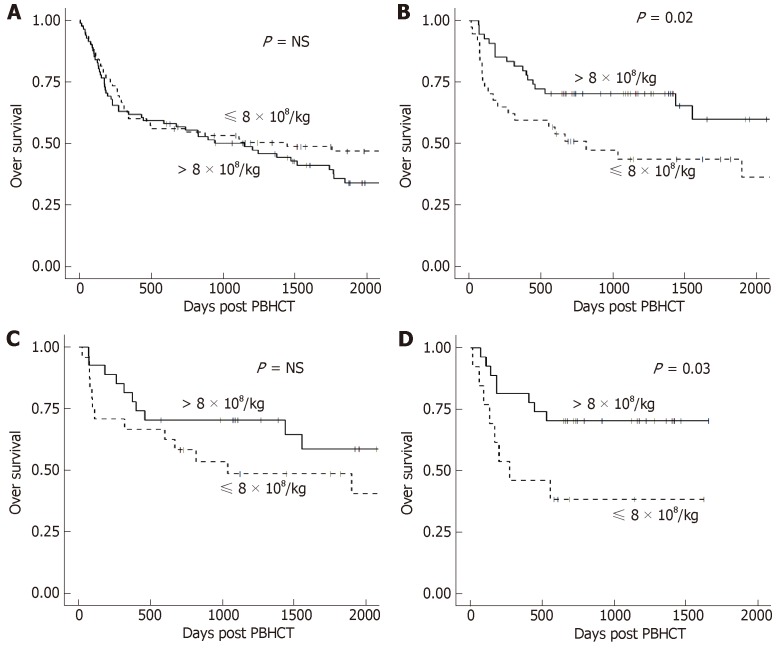
Neutrophil engraftment was significantly faster after reduced intensity TBI based conditioning [reduced intensity conditioning (RIC) + TBI] and > 4 × 10 CD34+ cells/kg infused. A higher total nucleated cell dose led to a higher incidence of grade II-IV acute graft-versus-host disease in the myeloablative + TBI regimen group ( = 0.03), but no significant difference in grade III-IV graft-versus-host disease. A higher total nucleated cell dose was also associated with increased incidence of moderate/severe chronic graft-versus-host disease, regardless of conditioning regimen. Overall and progression-free survival were significantly better in patients with a RIC + TBI regimen and total nucleated cell dose > 8 × 10/kg (3 years, overall survival: 70% 38%, = 0.02, 3 years, progression free survival: 64% 38%, = 0.02).
TBI and conditioning intensity may alter the relationship between infused cell doses and outcomes after PBHCT. Immune cell subsets may predict improved survival after unmanipulated PBHCT.
研究外周血造血细胞移植(PBHCT)后,输注的造血细胞剂量及其与预处理方案强度±全身照射(TBI)之间的相互作用对预后的影响。
我们的回顾性队列研究纳入了247例接受首次、T细胞充足、人类白细胞抗原匹配的异基因PBHCT且于2001年至2012年间接受治疗的患者。使用Pearson积矩相关系数计算相关性。采用Kaplan-Meier法生成总生存曲线和无进展生存曲线,并使用对数秩检验进行比较。
在基于TBI的减低强度预处理[减低强度预处理(RIC)+TBI]且输注>4×10⁶ CD34⁺细胞/kg后,中性粒细胞植入明显更快。在清髓性+TBI方案组中,较高的总核细胞剂量导致II-IV级急性移植物抗宿主病的发生率更高(P = 0.03),但III-IV级移植物抗宿主病无显著差异。无论预处理方案如何,较高的总核细胞剂量也与中/重度慢性移植物抗宿主病的发生率增加相关。采用RIC+TBI方案且总核细胞剂量>8×10⁸/kg的患者的总生存和无进展生存明显更好(3年总生存:70% 对38%,P = 0.02;3年无进展生存:64% 对38%,P = 0.02)。
TBI和预处理强度可能会改变PBHCT后输注细胞剂量与预后之间的关系。免疫细胞亚群可能预测未处理的PBHCT后的生存改善情况。