Department of Ophthalmology, Tri-Service General Hospital, National Defense Medical Center, Taipei 114, Taiwan.
Graduate Institute of Medical Sciences, National Defense Medical Center, Taipei 114, Taiwan.
Nutrients. 2019 Feb 27;11(3):509. doi: 10.3390/nu11030509.
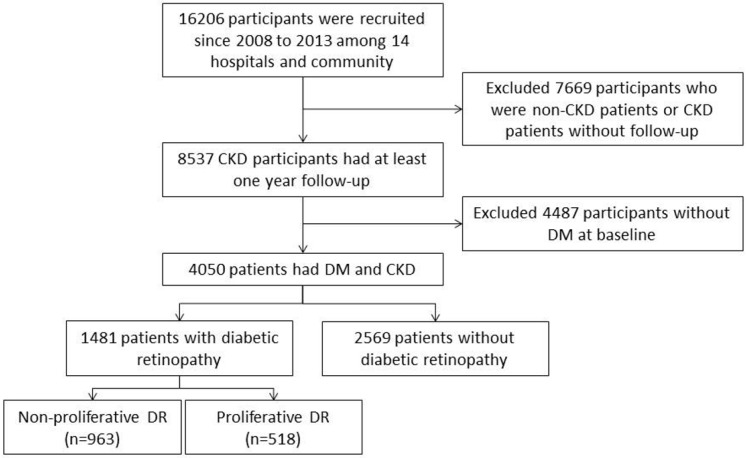
It has rarely been studied whether the presence and severity of diabetic retinopathy (DR) could influence the renal disease progression among all chronic kidney disease (CKD) diabetic patients. This study investigates the characteristics of diabetic patients, with different stages of chronic kidney disease (CKD), according to the occurrence of diabetic retinopathy and determines the influence of retinopathy in the deterioration of renal function. We conduct a multicenter, longitudinal cohort study based on the Epidemiology and Risk Factors Surveillance of the CKD project (2008⁻2013) and the National Health Insurance Research Database (NHIRD) (2001⁻2013). A total of 4050 diabetic patients with CKD, 20⁻85 years of age, from 14 hospitals and the community are included in this study. As compared to CKD patients without DR, CKD patients with DR have a lower baseline estimated glomerular filtration rate (eGFR) (39.17 ± 30.36 mL/min per 1.73 m² vs. 54.38 ± 33.67 mL/min per 1.73 m² ); poorer glycemic control (higher glycated hemoglobin (HbA1c) 7.85 ± 4.97 vs. 7.29 ± 4.02, < 0.01); higher proteinuria (urine protein-to-creatinine ratio (UPCR )1.94 ± 2.96 g/dL vs. 0.91 ± 2.11 g/dL, < 0.01); more anemia (Hb 11.22 ± 2.43 g/dL vs. 12.39 ± 3.85 g/dL, < 0.01), and more hypoalbuminemia (3.88 ± 0.95 g/dL vs. 4.16 ± 1.74 g/dL, < 0.01). Later stage (stage 3b⁻5) CKD patients with DR had significantly higher CKD progression compared with patients without DR (OR (odds ratio) 1.66 (1.36⁻2.02)). Patients with proliferative DR had significantly higher CKD progression events compared to patients with non-proliferative DR (OR 2.18 (1.71⁻2.78)). The presence and severity of DR is a risk factor for CKD progression among our Taiwanese CKD patients with diabetes. Prevention and early detection of DR are important and DR should be routinely screened as early as possible among diabetic CKD patients.
糖尿病视网膜病变(DR)的发生和严重程度是否会影响所有慢性肾脏病(CKD)糖尿病患者的肾脏疾病进展,这一问题很少得到研究。本研究调查了不同 CKD 阶段(根据 DR 的发生情况进行划分)糖尿病患者的特征,并确定了 DR 对肾功能恶化的影响。我们进行了一项基于 2008-2013 年肾脏病流行病学及危险因素监测项目(Epidemiology and Risk Factors Surveillance of the CKD project)和 2001-2013 年全民健康保险研究数据库(National Health Insurance Research Database)的多中心、纵向队列研究。共纳入来自 14 家医院和社区的 4050 名年龄在 20-85 岁之间、患有 CKD 的糖尿病患者。与无 DR 的 CKD 患者相比,有 DR 的 CKD 患者的基线估计肾小球滤过率(eGFR)更低(39.17 ± 30.36 mL/min/1.73 m² vs. 54.38 ± 33.67 mL/min/1.73 m²);血糖控制更差(糖化血红蛋白(HbA1c)更高,为 7.85 ± 4.97 vs. 7.29 ± 4.02, < 0.01);蛋白尿更多(尿蛋白与肌酐比值(UPCR)更高,为 1.94 ± 2.96 g/dL vs. 0.91 ± 2.11 g/dL, < 0.01);贫血更严重(Hb 更低,为 11.22 ± 2.43 g/dL vs. 12.39 ± 3.85 g/dL, < 0.01);低白蛋白血症更常见(3.88 ± 0.95 g/dL vs. 4.16 ± 1.74 g/dL, < 0.01)。与无 DR 的患者相比,DR 晚期(3b-5 期)CKD 患者的 CKD 进展明显更高(比值比(OR)为 1.66(1.36-2.02))。与非增殖性 DR 患者相比,增殖性 DR 患者的 CKD 进展事件明显更高(OR 为 2.18(1.71-2.78))。DR 的存在和严重程度是我们台湾地区糖尿病 CKD 患者 CKD 进展的危险因素。预防和早期发现 DR 非常重要,应尽早对糖尿病 CKD 患者进行常规筛查。