Division of Hematology/Oncology, Vanderbilt University Medical Center, Nashville, Tennessee, USA
Division of Hematology/Oncology, Vanderbilt University Medical Center, Nashville, Tennessee, USA.
Oncologist. 2019 May;24(5):584-588. doi: 10.1634/theoncologist.2018-0574. Epub 2019 Feb 28.
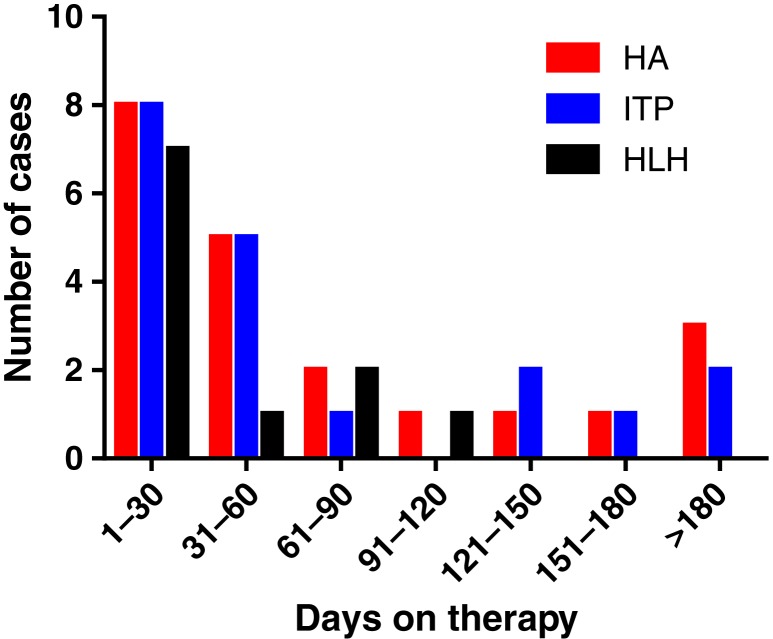
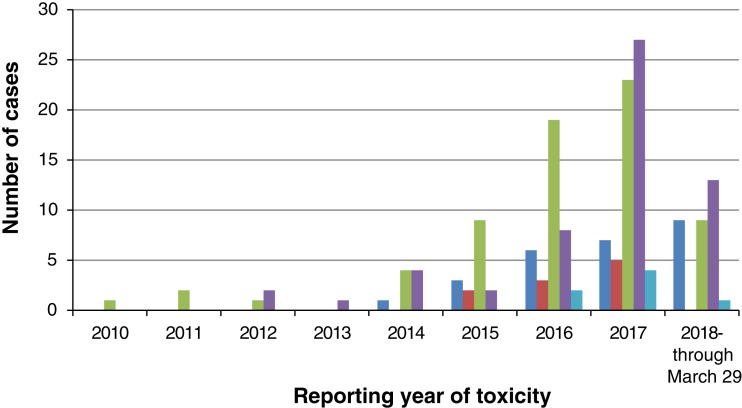
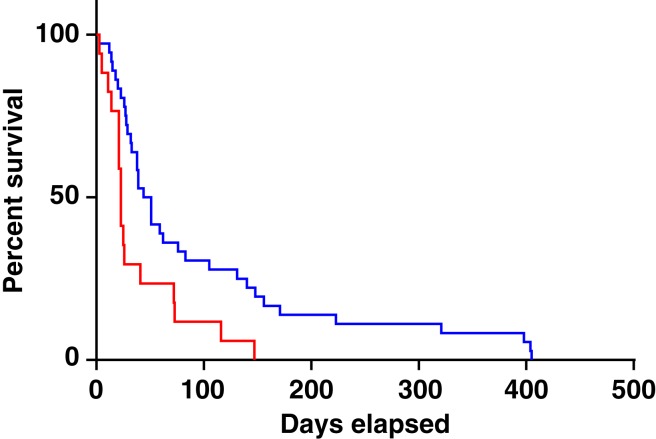
Immune checkpoint inhibitors have improved outcomes for patients with numerous hematological and solid cancers. Hematologic toxicities have been described, but the spectrum, timing, and clinical presentation of these complications are not well understood. We used the World Health Organization's pharmacovigilance database of individual-case-safety-reports (ICSRs) of adverse drug reactions, VigiBase, to identify cases of hematologic toxicities complicating immune checkpoint inhibitor therapy. We identified 168 ICSRs of immune thrombocytopenic purpura (ITP), hemolytic anemia (HA), hemophagocytic lymphohistiocytosis, aplastic anemia, and pure red cell aplasia in 164 ICSRs. ITP ( = 68) and HA ( = 57) were the most common of these toxicities and occurred concomitantly in four patients. These events occurred early on treatment (median 40 days) and were associated with fatal outcome in 12% of cases. Ipilimumab-based therapy (monotherapy or combination with anti-programmed death-1 [PD-1]) was associated with earlier onset (median 23 vs. 47.5 days, = .006) than anti-PD-1/programmed death ligand-1 monotherapy. Reporting of hematologic toxicities has increased over the past 2 years (98 cases between January 2017 and March 2018 vs. 70 cases before 2017), possibly because of increased use of checkpoint inhibitors and improved recognition of toxicities. Future studies should evaluate incidence of hematologic toxicities, elucidate risk factors, and determine the most effective treatment algorithms. KEY POINTS: Immune-mediated hematologic toxicities are a potential side effect of immune checkpoint inhibitors (ICIs).Providers should monitor complete blood counts during treatment with ICIs.Corticosteroids are the mainstay of treatment for immune-mediated hematologic toxicities.Further research is needed to define patient-specific risk factors and optimal management strategies for hematologic toxicities.
免疫检查点抑制剂改善了许多血液系统和实体瘤患者的预后。已经描述了血液学毒性,但这些并发症的谱、时间和临床表现尚不清楚。我们使用世界卫生组织的药物不良反应个体病例安全报告(ICSR)的药物警戒数据库(VigiBase)来识别免疫检查点抑制剂治疗中并发血液学毒性的病例。我们在 164 份 ICSR 中发现了 168 例免疫性血小板减少性紫癜(ITP)、溶血性贫血(HA)、噬血细胞性淋巴组织细胞增生症、再生障碍性贫血和纯红细胞再生障碍的 ICSR。其中 ITP( = 68)和 HA( = 57)是最常见的毒性,有 4 例患者同时发生这两种毒性。这些事件发生在治疗早期(中位数 40 天),在 12%的病例中与致命结局相关。基于伊匹单抗的治疗(单药或与抗程序性死亡-1[PD-1]联合)与抗 PD-1/程序性死亡配体-1 单药治疗相比,发病更早(中位数 23 天与 47.5 天, = .006)。在过去的 2 年中,血液学毒性的报告有所增加(2017 年 1 月至 2018 年 3 月期间有 98 例,而 2017 年之前有 70 例),这可能是由于检查点抑制剂的使用增加和毒性的识别改善。未来的研究应评估血液学毒性的发生率,阐明危险因素,并确定最有效的治疗方案。关键点:免疫介导的血液学毒性是免疫检查点抑制剂(ICI)的潜在副作用。治疗期间,临床医生应监测全血细胞计数。皮质类固醇是治疗免疫介导的血液学毒性的主要方法。需要进一步研究以确定血液学毒性的患者特异性危险因素和最佳管理策略。