Heart Failure Unit, Department of Cardiology, Hospital del Mar, Barcelona, Spain.
Heart Diseases Biomedical Research Group (GREC), IMIM (Hospital del Mar Medical Research Institute), Barcelona, Spain.
BMJ Open. 2017 Dec 21;7(12):e018719. doi: 10.1136/bmjopen-2017-018719.
The aim of this study was to analyse baseline characteristics and outcome of patients with heart failure and mid-range left ventricular ejection fraction (HFmrEF, left ventricular ejection fraction (LVEF) 40%-49%) and the effect of 1-year change in LVEF in this group.
Multicentre prospective observational study of ambulatory patients with HF followed up at four university hospitals with dedicated HF units.
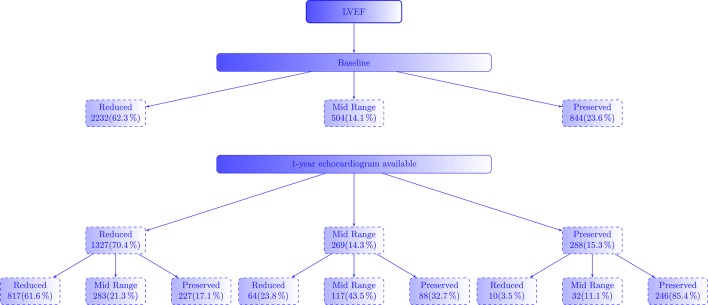
Fourteen per cent (n=504) of the 3580 patients included had HFmrEF.
Baseline characteristics, 1-year LVEF and outcomes were collected. All-cause death, HF hospitalisation and the composite end-point were the primary outcomes.
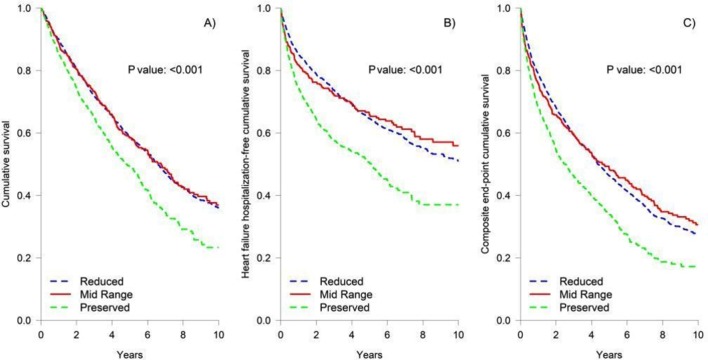
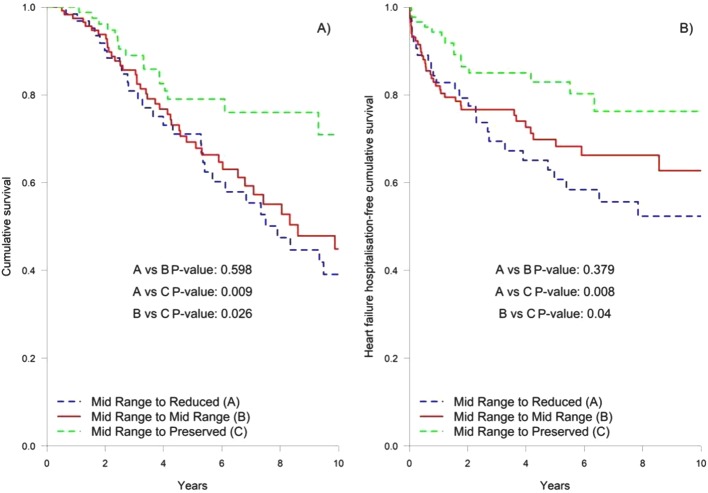
Median follow-up was 3.66 (1.69-6.04) years. All-cause death, HF hospitalisation and the composite end-point were 47%, 35% and 59%, respectively. Outcomes were worse in HF with preserved ejection fraction (HFpEF) (LVEF>50%), without differences between HF with reduced ejection fraction (HFrEF) (LVEF<40%) and HFmrEF (all-cause mortality 52.6% vs 45.8% and 43.8%, respectively, P=0.001). After multivariable Cox regression analyses, no differences in all-cause death and the composite end-point were seen between the three groups. HF hospitalisation and cardiovascular death were not statistically different between patients with HFmrEF and HFrEF. At 1-year follow-up, 62% of patients with HFmrEF had LVEF measured: 24% had LVEF<40%, 43% maintained LVEF 40%-49% and 33% had LVEF>50%. While change in LVEF as continuous variable was not associated with better outcomes, those patients who evolved from HFmrEF to HFpEF did have a better outcome. Those who remained in the HFmrEF and HFrEF groups had higher all-cause mortality after adjustment for age, sex and baseline LVEF (HR 1.96 (95% CI 1.08 to 3.54, P=0.027) and HR 2.01 (95% CI 1.04 to 3.86, P=0.037), respectively).
Patients with HFmrEF have a clinical profile in-between HFpEF and HFrEF, without differences in all-cause mortality and the composite end-point between the three groups. At 1 year, patients with HFmrEF exhibited the greatest variability in LVEF and this change was associated with survival.
本研究旨在分析射血分数中间值心力衰竭(HFmrEF,左心室射血分数(LVEF)为 40%-49%)患者的基线特征和结局,并探讨该组患者 LVEF 1 年变化的影响。
对四家设有专门心力衰竭病房的大学附属医院的门诊心力衰竭患者进行的多中心前瞻性观察性研究。
在纳入的 3580 名患者中,有 14%(n=504)为 HFmrEF。
收集基线特征、1 年 LVEF 和结局。全因死亡、心力衰竭住院和复合终点为主要结局。
中位随访时间为 3.66(1.69-6.04)年。全因死亡、心力衰竭住院和复合终点的发生率分别为 47%、35%和 59%。射血分数保留型心力衰竭(HFpEF,LVEF>50%)患者的结局更差,射血分数降低型心力衰竭(HFrEF,LVEF<40%)和 HFmrEF 之间无差异(全因死亡率分别为 52.6%、45.8%和 43.8%,P=0.001)。多变量 Cox 回归分析后,三组间全因死亡和复合终点无差异。HFmrEF 和 HFrEF 患者的心力衰竭住院和心血管死亡无统计学差异。在 1 年随访时,有 62%的 HFmrEF 患者测量了 LVEF:24%的患者 LVEF<40%,43%的患者维持 LVEF 40%-49%,33%的患者 LVEF>50%。虽然 LVEF 作为连续变量的变化与更好的结局无关,但从 HFmrEF 转为 HFpEF 的患者结局更好。那些仍处于 HFmrEF 和 HFrEF 组的患者,在调整年龄、性别和基线 LVEF 后,全因死亡率更高(HR 1.96(95%CI 1.08 至 3.54,P=0.027)和 HR 2.01(95%CI 1.04 至 3.86,P=0.037))。
HFmrEF 患者的临床特征介于 HFpEF 和 HFrEF 之间,三组间全因死亡率和复合终点无差异。在 1 年时,HFmrEF 患者的 LVEF 变化最大,且这种变化与生存相关。