Department of Radiology, Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Harvard Medical School, Charlestown, MA, United States.
Division of Clinical Research, Korea Institute of Oriental Medicine, Daejeon, Korea.
Pain. 2019 Jul;160(7):1594-1605. doi: 10.1097/j.pain.0000000000001541.
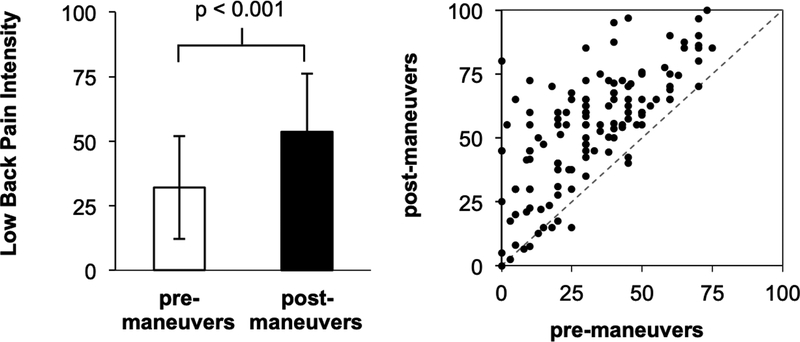
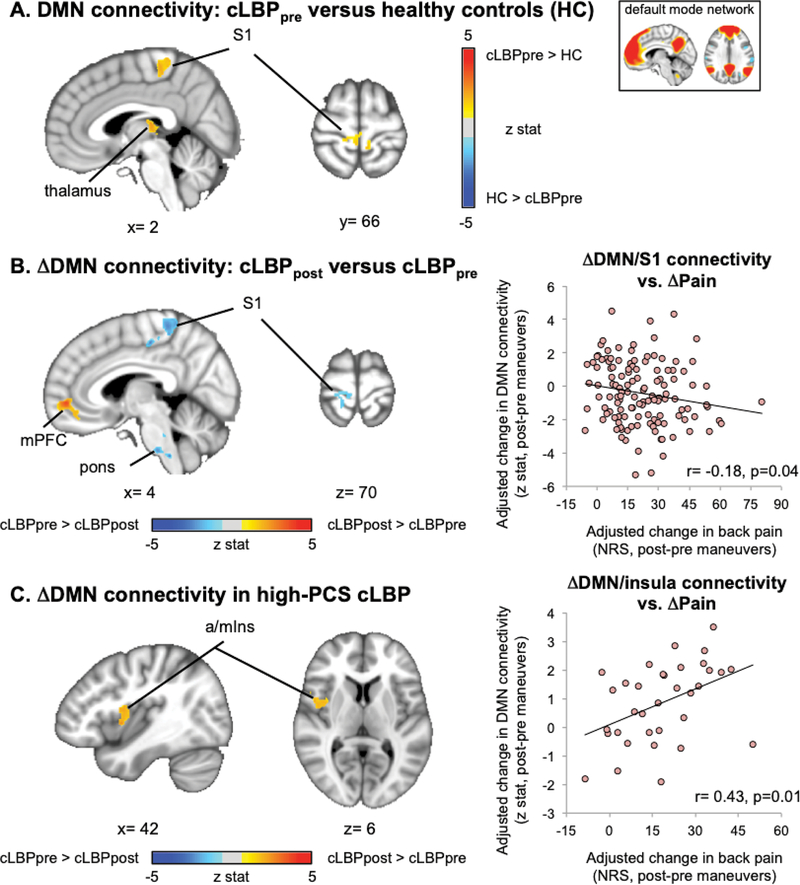
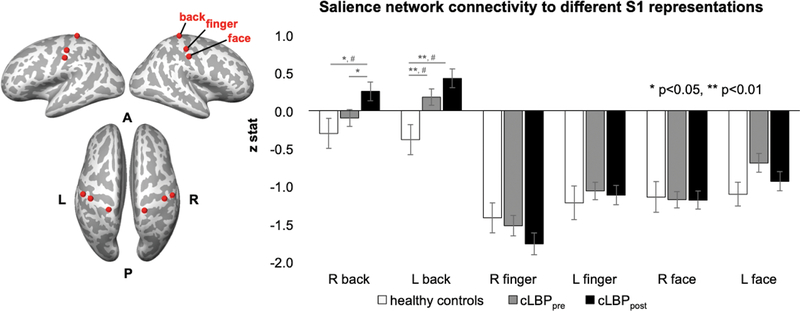
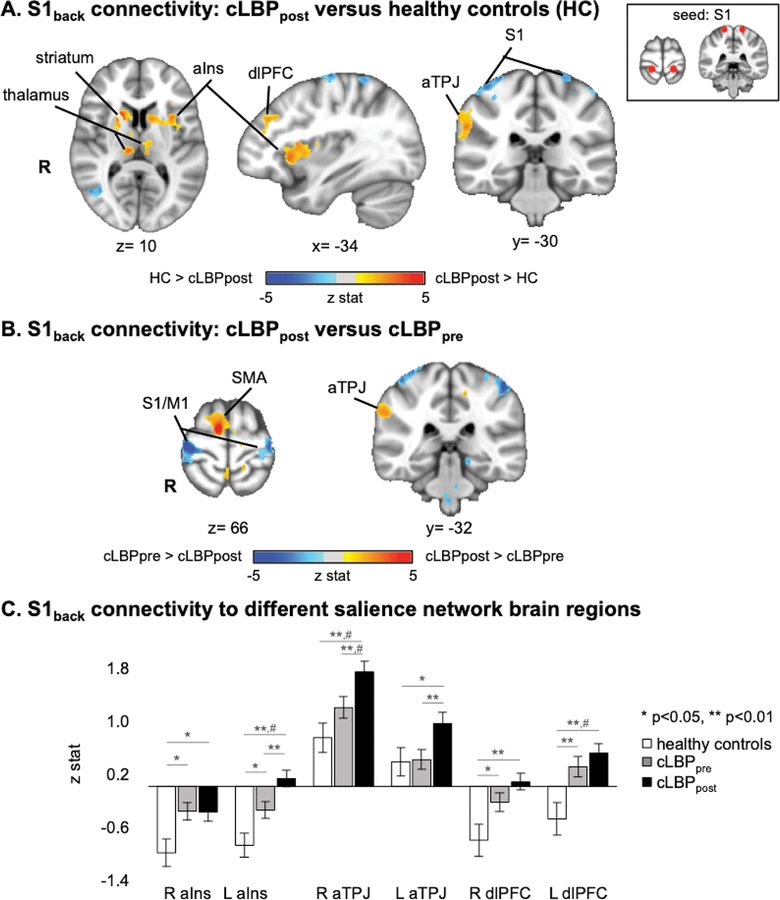
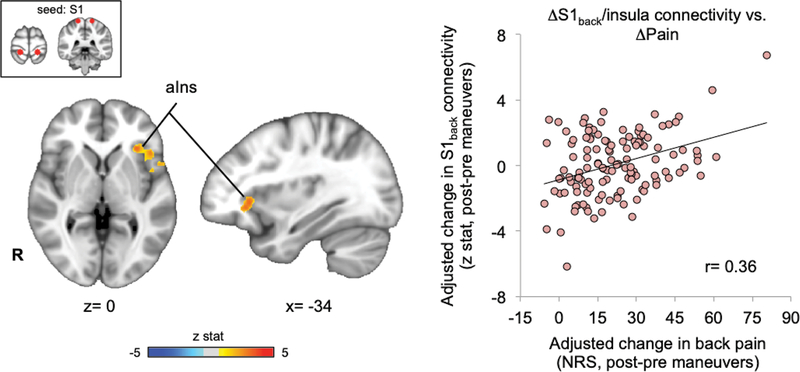
Although several studies have found that chronic pain is characterized by increased cross-network connectivity between salience network, sensorimotor network, and default mode network (DMN), a large sample-size investigation allowing for a more reliable evaluation of somatotopic specificity and subgroup analyses with linkage to clinical pain intensity has been lacking. We enrolled healthy adults and a large cohort of patients (N = 181) suffering from chronic low back pain (cLBP). To specifically link brain connectivity with clinical pain intensity, patients were scanned at baseline and after performing physical maneuvers that exacerbated pain. Compared with healthy adults, patients with cLBP demonstrated increased connectivity between the functionally localized back representation in the primary somatosensory cortex (S1back) and both salience network and DMN. Pain exacerbation maneuvers increased S1back connectivity to salience network regions, but decreased connectivity to DMN, with greater pain intensity increase associated with greater shifts in these connectivity patterns. Furthermore, only in patients with cLBP reporting high pain catastrophizing, DMN connectivity was increased to a cardinal node of the salience network, anterior insula cortex, which was correlated with increased postmaneuver pain in this cLBP subgroup. Hence, increased information transfer between salience processing regions, particularly anterior insula, and DMN may be strongly influenced by pain catastrophizing. Increased information transfer between the salience network and S1 likely plays an important role in shifting nociceptive afference away from self-referential processing, reallocating attentional focus, and affective coding of nociceptive afference from specific body areas. These results demonstrate S1 somatotopic specificity for cross-network connectivity in encoding clinical back pain and moderating influence of catastrophizing for DMN/insula connectivity.
尽管有几项研究发现,慢性疼痛的特征是显著网络、感觉运动网络和默认模式网络(DMN)之间的跨网络连接增加,但缺乏大样本量的研究来更可靠地评估躯体特定性和与临床疼痛强度相关的亚组分析。我们招募了健康成年人和一大群患有慢性下腰痛(cLBP)的患者(N=181)。为了将大脑连接与临床疼痛强度具体联系起来,患者在基线时和进行加重疼痛的身体动作后进行了扫描。与健康成年人相比,cLBP 患者的初级体感皮层(S1back)中功能定位的背部代表区域与显著网络和 DMN 之间的连接增加。疼痛加重动作增加了 S1back 与显著网络区域的连接,但减少了与 DMN 的连接,疼痛强度增加与这些连接模式的更大变化相关。此外,只有在报告高疼痛灾难化的 cLBP 患者中,DMN 与显著网络的核心节点,前岛叶皮层的连接增加,这与该 cLBP 亚组中手术后疼痛增加相关。因此,显著处理区域(特别是前岛叶)和 DMN 之间的信息传递增加可能受到疼痛灾难化的强烈影响。显著网络和 S1 之间的信息传递增加可能在将伤害性传入信息从自我参照处理中转移、重新分配注意力焦点以及对来自特定身体区域的伤害性传入信息进行情感编码方面发挥重要作用。这些结果表明 S1 在编码临床腰痛的跨网络连接中具有躯体特定性,并且灾难化对 DMN/岛叶连接具有调节作用。