Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women's Hospital, Harvard Medical School (HMS), Boston, MA, USA Department of Psychiatry, Massachusetts General Hospital, HMS, Boston, MA, USA MGH/MIT/HMS Athinoula A. Martinos Center for Biomedical Imaging, Charlestown, MA, USA Program in Placebo Studies & the Therapeutic Encounter, Beth Israel Deaconess Medical Center, HMS, Boston, MA, USA Department of Psychiatry, Brigham and Women's Hospital, HMS, Boston, MA, USA.
Pain. 2013 Jan;154(1):24-33. doi: 10.1016/j.pain.2012.07.029. Epub 2012 Oct 27.
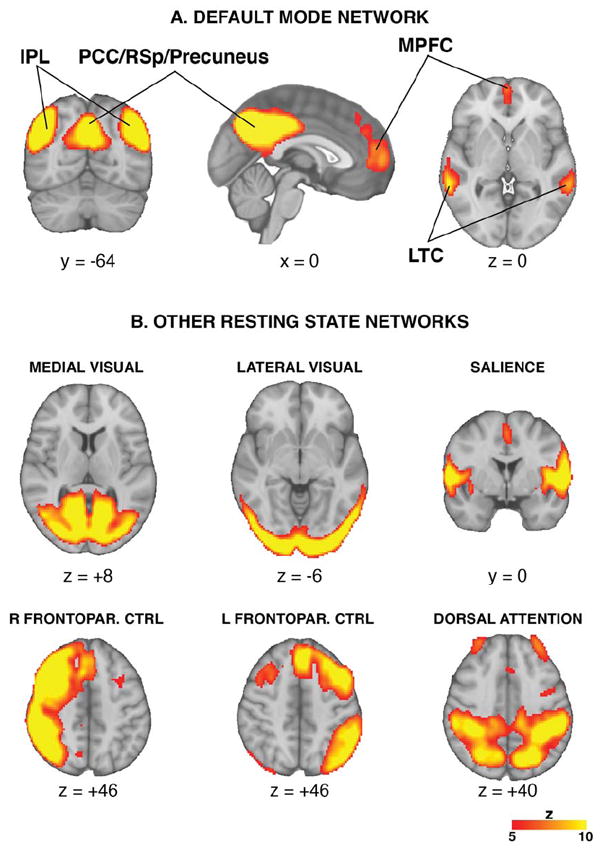
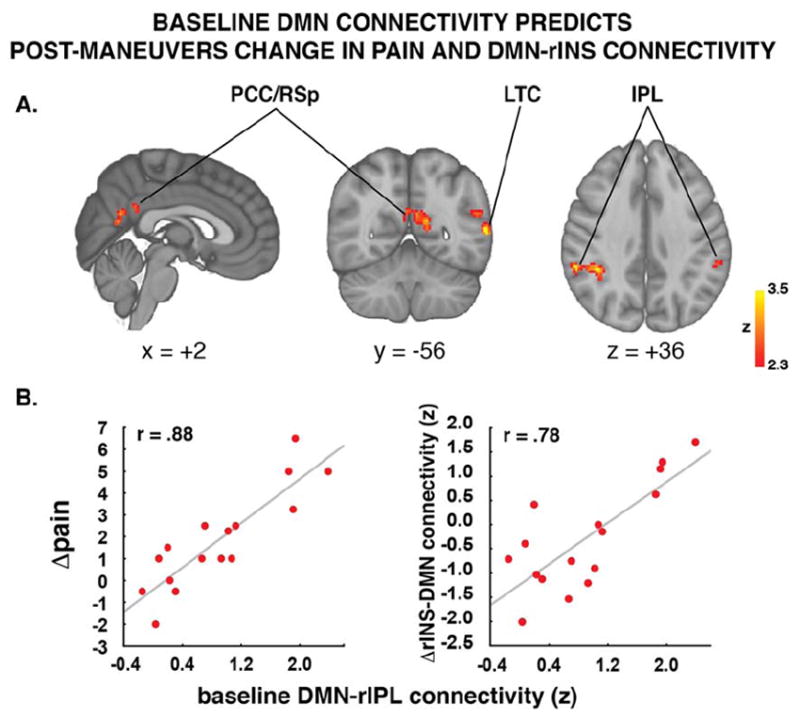
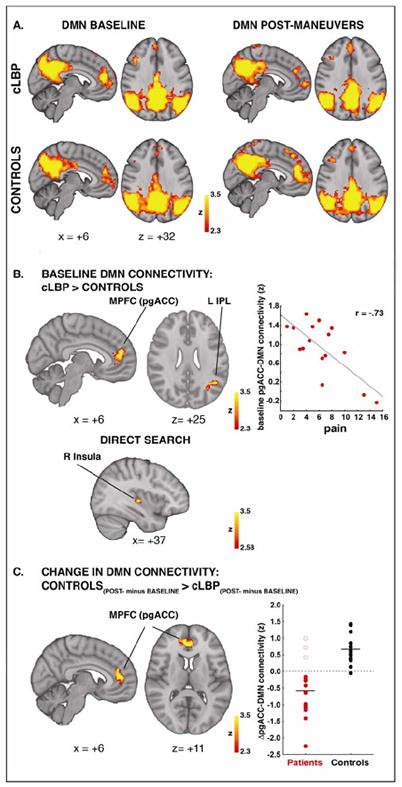
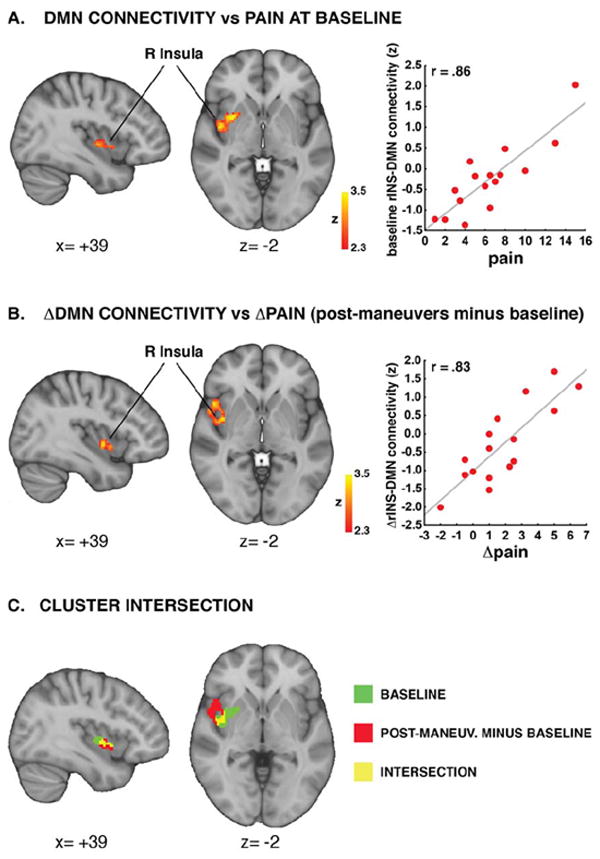
Neuroimaging studies have suggested the presence of alterations in the anatomo-functional properties of the brain of patients with chronic pain. However, investigation of the brain circuitry supporting the perception of clinical pain presents significant challenges, particularly when using traditional neuroimaging approaches. While potential neuroimaging markers for clinical pain have included resting brain connectivity, these cross-sectional studies have not examined sensitivity to within-subject exacerbation of pain. We used the dual regression probabilistic Independent Component Analysis approach to investigate resting-state connectivity on arterial spin labeling data. Brain connectivity was compared between patients with chronic low back pain (cLBP) and healthy controls, before and after the performance of maneuvers aimed at exacerbating clinical pain levels in the patients. Our analyses identified multiple resting state networks, including the default mode network (DMN). At baseline, patients demonstrated stronger DMN connectivity to the pregenual anterior cingulate cortex (pgACC), left inferior parietal lobule, and right insula (rINS). Patients' baseline clinical pain correlated positively with connectivity strength between the DMN and right insula (DMN-rINS). The performance of calibrated physical maneuvers induced changes in pain, which were paralleled by changes in DMN-rINS connectivity. Maneuvers also disrupted the DMN-pgACC connectivity, which at baseline was anticorrelated with pain. Finally, baseline DMN connectivity predicted maneuver-induced changes in both pain and DMN-rINS connectivity. Our results support the use of arterial spin labeling to evaluate clinical pain, and the use of resting DMN connectivity as a potential neuroimaging biomarker for chronic pain perception.
神经影像学研究表明,慢性疼痛患者的大脑解剖功能特性存在改变。然而,对支持临床疼痛感知的大脑回路进行研究具有很大的挑战性,特别是在使用传统神经影像学方法的情况下。尽管潜在的临床疼痛神经影像学标志物包括静息脑连接,但这些横断面研究并未检查对疼痛加剧的敏感性。我们使用双回归概率独立成分分析方法来研究动脉自旋标记数据的静息状态连接。在患者进行旨在加剧临床疼痛水平的操作之前和之后,比较了慢性下腰痛(cLBP)患者和健康对照组之间的大脑连接。我们的分析确定了多个静息状态网络,包括默认模式网络(DMN)。在基线时,患者表现出更强的 DMN 连接到前扣带回皮质的前下(pgACC)、左顶下小叶和右侧岛叶(rINS)。患者的基线临床疼痛与 DMN 与右侧岛叶(DMN-rINS)之间的连接强度呈正相关。经过校准的物理操作会引起疼痛变化,同时 DMN-rINS 连接也会发生变化。操作还破坏了 DMN-pgACC 连接,基线时该连接与疼痛呈负相关。最后,基线 DMN 连接可预测疼痛和 DMN-rINS 连接变化。我们的结果支持使用动脉自旋标记来评估临床疼痛,并支持将静息 DMN 连接用作慢性疼痛感知的潜在神经影像学生物标志物。