Department of Medical Oncology, Institute of Oncology Ljubljana, Ljubljana, Slovenia.
Radiol Oncol. 2019 Mar 3;53(1):85-95. doi: 10.2478/raon-2019-0013.
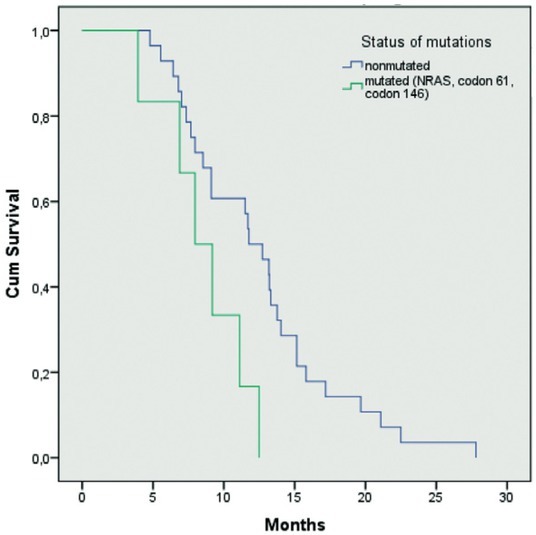
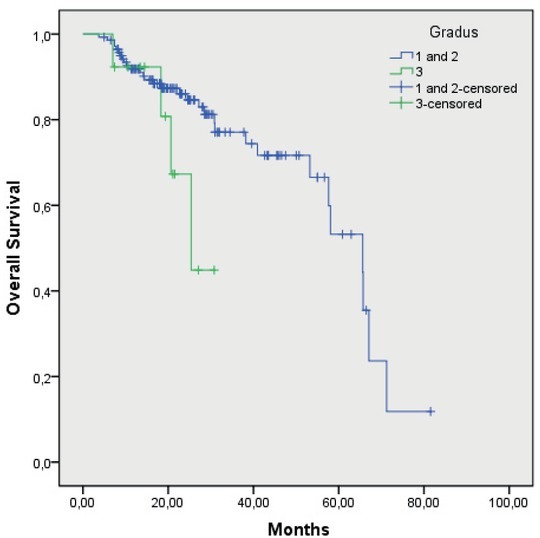
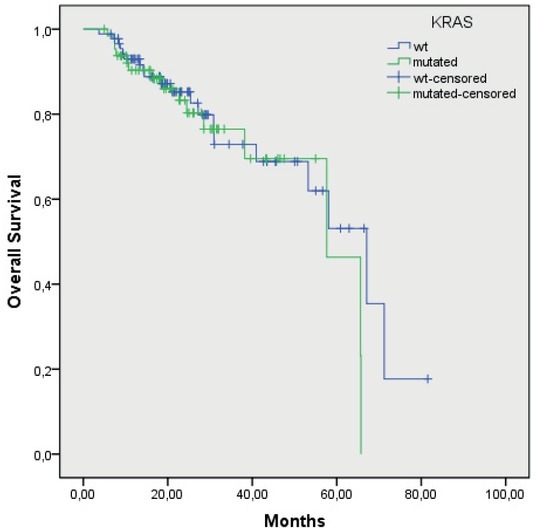
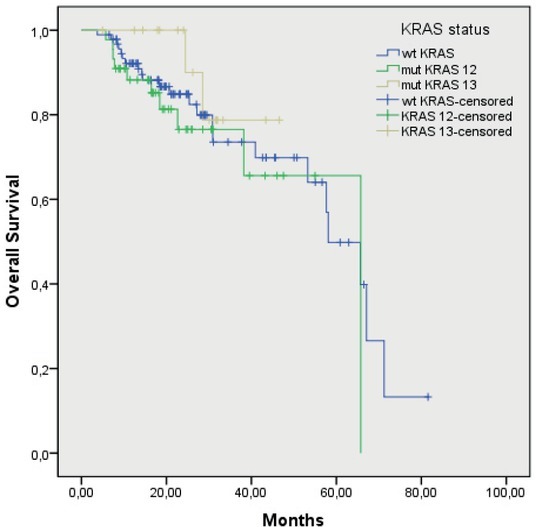
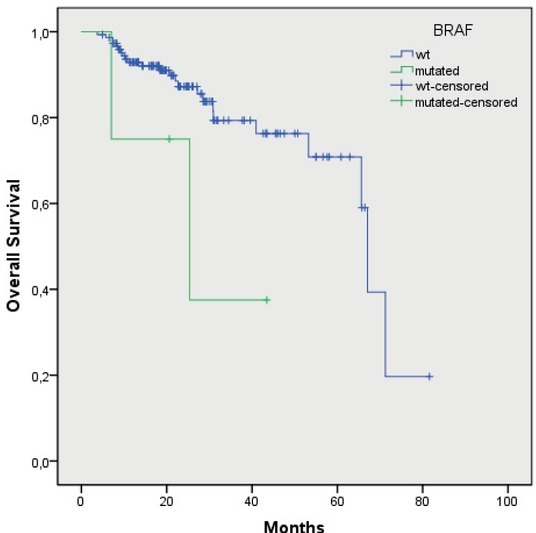
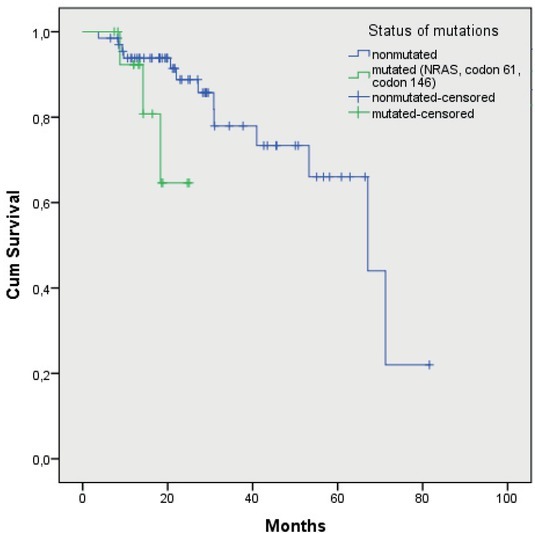
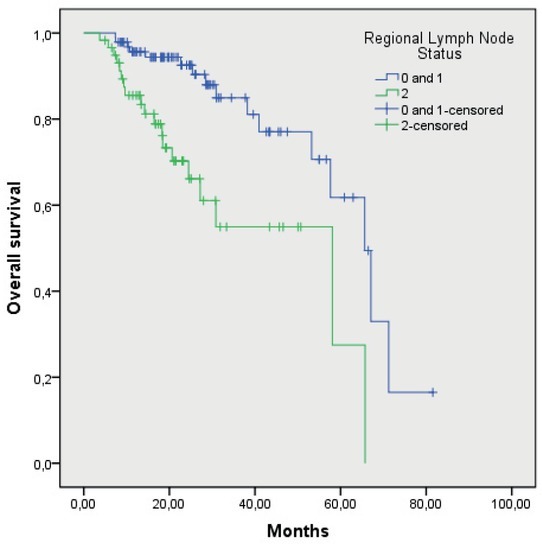
Background Histological parameters of primary tumour and nodal metastases are prognostic factors for survival of operable colorectal (CRC) patients, but not predictive for response rate of systemic therapy. KRAS mutations in codons 12 and 13 were first recognized as a predictive factor for resistance to anti-EGFR monoclonal antibodies. Not all patients with wild-type KRAS (wtKRAS) respond to anti-EGFR antibody treatment. Additional mechanisms of resistance may activate mutations of the other main EGFR effectors pathway, such as other mutations in RAS gene, mutations in P13K and PTEN expression. Patients and methods In the prospective study prognostic and predictive impact of histological parameters of primary tumour, KRAS and BRAF mutations on overall survival (OS) and objective response (OR) rate of metastatic CRC (mCRC) patients treated with 1st line systemic therapy were analysed. We additionally retrospectively analysed other mutations in RAS genes and their impact on survival and time to progression. Results From November 2010 to December 2012, we enrolled 154 patients in the study, 95 men and 59 women. Mutations in KRAS gene and V600E BRAF gene were found in 42% and in 3% of patients, respectively. Median OS of the patients with T1, T2 and T3 tumour was 65.4 months (95% CI, 55.7-75.6) while in patients with T4 tumour, lymphangiosis, vascular and perineural invasion it has not been reached yet. Median OS of the patients with G1, G2 and G3 of tumour differentiation was 65.6 (95% CI, 53.7-77.5) and 25.3 months (95% CI, 16.6-34.1), respectively. Median OS of the patients with stage N0, N1 and N2 was 65.6 (95% CI, 56.4-74.8) and 58.0 months (95% CI, 21.9-94.2), respectively. Median OS of wtKRAS and mutated KRAS patients was 56.5 (95% CI, 48.2-64.9) and 58 months (95% CI, 52.6-63.4), respectively. Median OS of mutated codon 12 and codon 13 patients was 57 (95% CI, 50.9-64.4) and 44 months (95% CI, 40.1-48.4), respectively. Median OS of wtBRAF and of mutated BRAF patients was 59.2 (95% CI, 52.5-65.9) and 27.6 months (95% CI, 12.6-42.5), respectively. wtKRAS significantly affected the response to the first systemic therapy (p = 0.028), while other parameters did not affected it, p= 0.07. In 14 patients (17%), additional mutations in NRAS gene, codon 61 and codon 146 were found. Median OS of wtNRAS, codon 61 and 146 patients was 67.1 months (50.3-67.6) while median OS of mutated NRAS patients has not been reached yet (p = 0.072). Median time to progression of wtNRAS, codon 61 and 146 patients was 11.7 months (10.4-14.5) while median time to progression of mutated NRAS patients was 7.9 months (6.1-11.0), (p = 0.025). Conclusions Mutated BRAF, N2 and G3 of primary tumour were poor prognostic factors for OS in mCRC patients. wtKRAS significantly affected the response to the first line systemic therapy. Histological parameters included in the analysis and mutated BRAF did not affect significantly the efficacy of 1st line systemic therapy in mCRC patients.
原发性肿瘤和淋巴结转移的组织学参数是可手术结直肠癌(CRC)患者生存的预后因素,但不是全身治疗反应率的预测因素。KRAS 密码子 12 和 13 的突变首先被认为是抗 EGFR 单克隆抗体耐药的预测因素。并非所有 KRAS 野生型(wtKRAS)的患者均对抗 EGFR 抗体治疗有反应。其他耐药机制可能会激活其他主要 EGFR 效应子通路的突变,例如 RAS 基因中的其他突变、PI3K 和 PTEN 表达的突变。
在这项前瞻性研究中,分析了原发性肿瘤、KRAS 和 BRAF 突变的组织学参数、对转移性 CRC(mCRC)患者一线系统治疗的总生存(OS)和客观缓解(OR)率的预后和预测影响。我们还回顾性分析了 RAS 基因的其他突变及其对生存和无进展时间的影响。
从 2010 年 11 月至 2012 年 12 月,我们招募了 154 名患者参加这项研究,其中 95 名男性,59 名女性。KRAS 基因和 V600E BRAF 基因的突变分别在 42%和 3%的患者中发现。T1、T2 和 T3 肿瘤患者的中位 OS 为 65.4 个月(95%CI,55.7-75.6),而 T4 肿瘤、淋巴管浸润、血管浸润和神经周围浸润的患者尚未达到。G1、G2 和 G3 肿瘤分化患者的中位 OS 分别为 65.6(95%CI,53.7-77.5)和 25.3 个月(95%CI,16.6-34.1)。N0、N1 和 N2 期患者的中位 OS 分别为 65.6(95%CI,56.4-74.8)和 58.0 个月(95%CI,21.9-94.2)。wtKRAS 和突变 KRAS 患者的中位 OS 分别为 56.5(95%CI,48.2-64.9)和 58 个月(95%CI,52.6-63.4)。突变密码子 12 和密码子 13 患者的中位 OS 分别为 57(95%CI,50.9-64.4)和 44 个月(95%CI,40.1-48.4)。wtBRAF 和突变 BRAF 患者的中位 OS 分别为 59.2(95%CI,52.5-65.9)和 27.6 个月(95%CI,12.6-42.5)。wtKRAS 显著影响一线系统治疗的反应(p = 0.028),而其他参数则没有影响(p = 0.07)。在 14 名患者(17%)中发现了 NRAS 基因、密码子 61 和 146 的额外突变。wtNRAS、密码子 61 和 146 患者的中位 OS 为 67.1 个月(50.3-67.6),而突变 NRAS 患者的中位 OS 尚未达到(p = 0.072)。wtNRAS、密码子 61 和 146 患者的中位无进展时间为 11.7 个月(10.4-14.5),而突变 NRAS 患者的中位无进展时间为 7.9 个月(6.1-11.0)(p = 0.025)。
BRAF 突变、N2 和 G3 是 mCRC 患者 OS 的不良预后因素。wtKRAS 显著影响一线系统治疗的反应。分析中包含的组织学参数和突变 BRAF 并未显著影响 mCRC 患者一线系统治疗的疗效。