Choi Yunsuk, Chung Sang Bong, Kim Myoung Soo
Department of Neurosurgery, National Medical Center, Seoul, Korea.
Brain Center, Pohang SM Christianity Hospital, Pohang, Korea.
J Korean Neurosurg Soc. 2019 Mar;62(2):175-182. doi: 10.3340/jkns.2018.0048. Epub 2019 Feb 27.
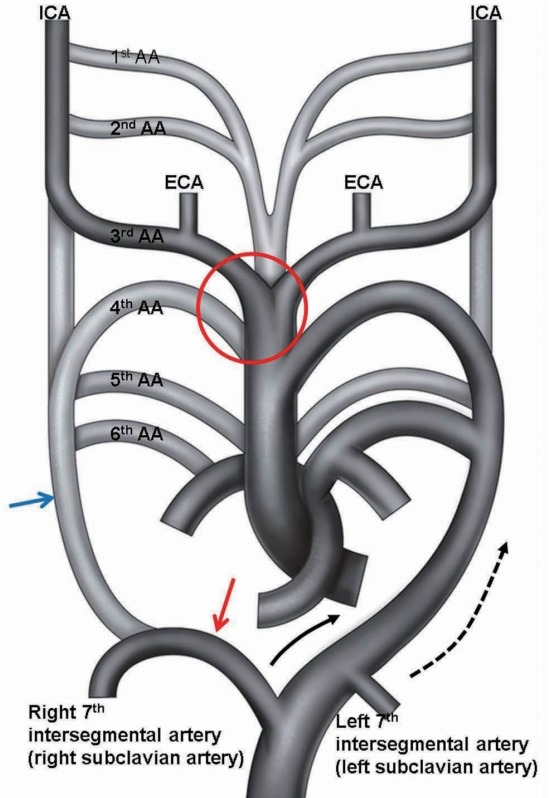
Aberrant right subclavian artery (ARSA) is a rare anatomical variant of the origin of the right subclavian artery. ARSA is defined as the right subclavian artery originating as the final branch of the aortic arch. The purpose of this study is to determine the prevalence and the anatomy of ARSA evaluated with computed tomography (CT) angiography.
CT angiography was performed in 3460 patients between March 1, 2014 and November 30, 2015 and the results were analyzed. The origin of the ARSA, course of the vessel, possible inadvertent ARSA puncture site during subclavian vein catheterization, Kommerell diverticula, and associated vascular anomalies were evaluated. We used the literature to review the clinical importance of ARSA.
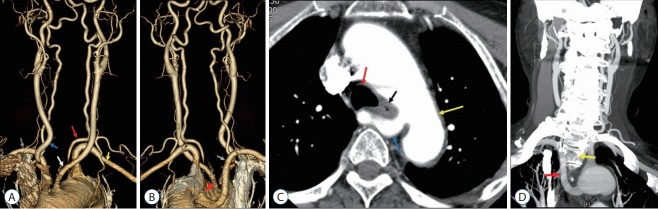
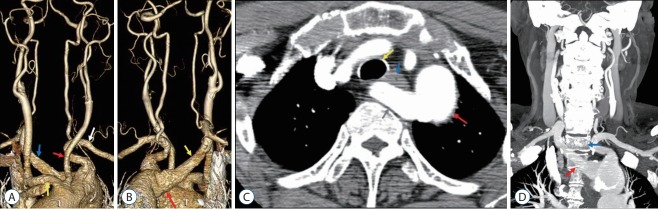
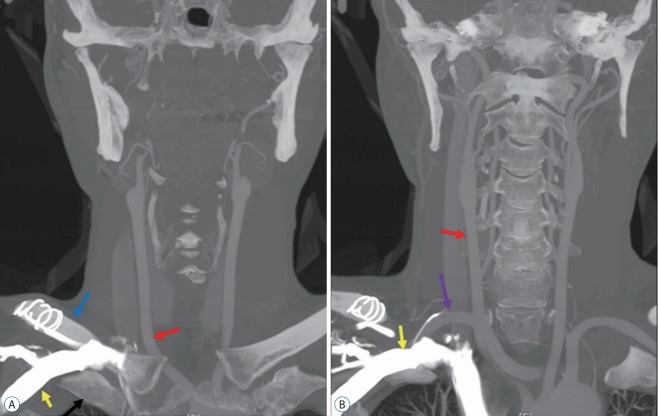
Seventeen in 3460 patients had ARSA. All ARSAs in 17 patients originated from the posterior aspect of the aortic arch and traveled along a retroesophageal course to the right thoracic outlet. All 17 ARSAs were located in the anterior portion from first to fourth thoracic vertebral bodies and were located near the right subclavian vein at the medial third of the clavicle. Only one of 17 patients presented with dysphagia.
It is important to be aware ARSA before surgical approaches to upper thoracic vertebrae in order to avoid complications and effect proper treatment. In patients with a known ARSA, a right transradial approach for aortography or cerebral angiography should be changed to a left radial artery or transfemoral approach.
异常右锁骨下动脉(ARSA)是右锁骨下动脉起源的一种罕见解剖变异。ARSA被定义为起源于主动脉弓终末分支的右锁骨下动脉。本研究的目的是确定通过计算机断层扫描(CT)血管造影评估的ARSA的患病率和解剖结构。
对2014年3月1日至2015年11月30日期间的3460例患者进行了CT血管造影,并对结果进行了分析。评估了ARSA的起源、血管走行、锁骨下静脉置管期间可能意外穿刺ARSA的部位、Kommerell憩室以及相关血管异常。我们查阅文献以回顾ARSA的临床重要性。
3460例患者中有17例患有ARSA。17例患者的所有ARSA均起源于主动脉弓后方,沿食管后走行至右胸廓出口。所有17条ARSA均位于第一至第四胸椎椎体的前部,在锁骨内侧三分之一处靠近右锁骨下静脉。17例患者中只有1例出现吞咽困难。
在上胸椎手术前了解ARSA很重要,以避免并发症并进行适当治疗。对于已知患有ARSA的患者,主动脉造影或脑血管造影的右桡动脉途径应改为左桡动脉或经股动脉途径。