MMWR Morb Mortal Wkly Rep. 2019 Mar 8;68(9):220-224. doi: 10.15585/mmwr.mm6809e2.
By 2007, all Department of Veterans Affairs medical centers (VAMCs) had initiated a multifaceted methicillin-resistant Staphylococcus aureus (MRSA) prevention program. MRSA and methicillin-susceptible S. aureus (MSSA) infection rates among VAMC inpatients from 2005 to 2017 were assessed.
Clinical microbiology data from any patient admitted to an acute-care VAMC in the United States from 2005 through 2017 and trends in hospital-acquired MRSA colonization were examined.
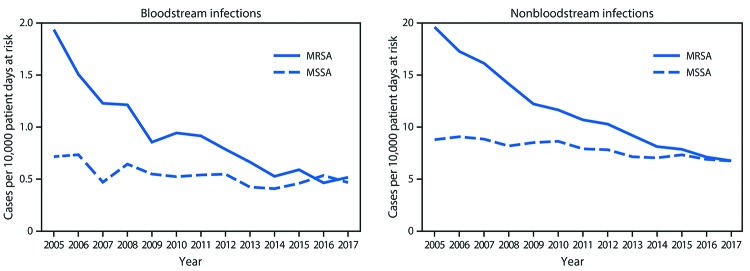
S. aureus infections decreased by 43% overall during the study period (p<0.001), driven primarily by decreases in MRSA, which decreased by 55% (p<0.001), whereas MSSA decreased by 12% (p = 0.003). Hospital-onset MRSA and MSSA infections decreased by 66% (p<0.001) and 19% (p = 0.02), respectively. Community-onset MRSA infections decreased by 41% (p<0.001), whereas MSSA infections showed no significant decline. Acquisition of MRSA colonization decreased 78% during 2008-2017 (17% annually, p<0.001). MRSA infection rates declined more sharply among patients who had negative admission surveillance MRSA screening tests (annual 9.7% decline) compared with those among patients with positive admission MRSA screening tests (4.2%) (p<0.05).
Significant reductions in S. aureus infection following the VAMC intervention were led primarily by decreases in MRSA. Moreover, MRSA infection declines were much larger among patients not carrying MRSA at the time of admission than among those who were. Taken together, these results suggest that decreased MRSA transmission played a substantial role in reducing overall S. aureus infections at VAMCs. Recent calls to withdraw infection control interventions designed to prevent MRSA transmission might be premature and inadvisable, at least until more is known about effective control of bacterial pathogen transmission in health care settings. Effective S. aureus prevention strategies require a multifaceted approach that includes adherence to current CDC recommendations for preventing not only device- and procedure-associated infections, but also transmission of health care-prevalent strains.
到 2007 年,所有退伍军人事务部医疗中心(VAMC)都启动了多方面的耐甲氧西林金黄色葡萄球菌(MRSA)预防计划。评估了 2005 年至 2017 年期间 VAMC 住院患者的 MRSA 和甲氧西林敏感金黄色葡萄球菌(MSSA)感染率。
从 2005 年至 2017 年期间,检查了任何在美国急性护理 VAMC 住院的患者的临床微生物学数据,以及医院获得性 MRSA 定植的趋势。
在研究期间,金黄色葡萄球菌感染总体下降了 43%(p<0.001),主要是由于 MRSA 下降了 55%(p<0.001),而 MSSA 下降了 12%(p = 0.003)。医院获得性 MRSA 和 MSSA 感染分别下降了 66%(p<0.001)和 19%(p = 0.02)。社区获得性 MRSA 感染下降了 41%(p<0.001),而 MSSA 感染没有明显下降。2008-2017 年间,MRSA 定植的获得减少了 78%(每年 17%,p<0.001)。与入院 MRSA 筛查检测阳性的患者相比,入院阴性监测 MRSA 筛查检测的患者的 MRSA 感染率下降更为明显(每年 9.7%的下降)(p<0.05)。
退伍军人事务部干预措施后,金黄色葡萄球菌感染显著减少,主要是由于 MRSA 减少。此外,在入院时未携带 MRSA 的患者中,MRSA 感染的下降幅度明显大于携带 MRSA 的患者。综上所述,这些结果表明,MRSA 传播的减少在退伍军人事务部医疗中心减少总体金黄色葡萄球菌感染方面发挥了重要作用。最近呼吁撤回旨在预防 MRSA 传播的感染控制干预措施可能为时过早且不可取,至少在了解卫生保健环境中细菌病原体传播的有效控制措施之前是这样。有效的金黄色葡萄球菌预防策略需要采取多方面的方法,包括遵守疾病预防控制中心目前关于预防不仅与设备和程序相关的感染,而且还预防卫生保健流行菌株传播的建议。