Nicol Martin, Baudet Mathilde, Cohen-Solal Alain
Lariboisiere/Saint Louis Hospital, Cardiology Department Paris, France.
UMR-S942 (BioCANVAS), Paris Diderot University Paris, France.
Card Fail Rev. 2019 Feb;5(1):31-36. doi: 10.15420/cfr.2018.25.1.
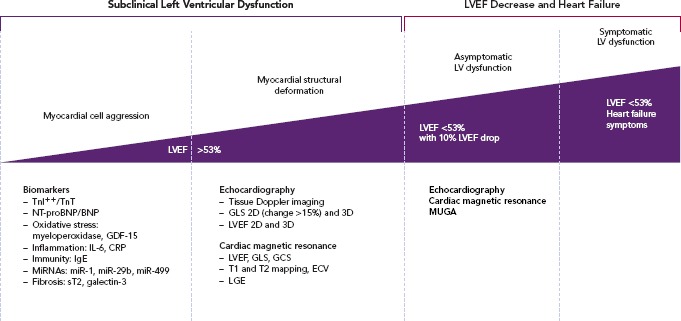
Subclinical left ventricular dysfunction is the most common cardiac complication after chemotherapy administration. Detection and early treatment are major issues for better cardiac outcomes in this cancer population. The most common definition of cardiotoxicity is a 10-percentage point decrease of left ventricular ejection fraction (LVEF) to a value <53%. The myocardial injury induced by chemotherapies is probably a continuum starting with cardiac biomarkers increase before the occurence of a structural myocardial deformation leading to a LVEF decline. An individualised risk profile (depending on age, cardiovascular risk factors, type of chemotherapy, baseline troponin, baseline global longitudinal strain and baseline LVEF) has to be determined before starting chemotherapy to consider cardioprotective treatment. To date, there is no proof of a systematic cardioprotective treatment (angiotensin-converting enzyme inhibitor and/or beta-blocker) in all cancer patients. However, early cardioprotective treatment in case of subclinical left ventricular dysfunction seems to be promising in the prevention of cardiac events.
亚临床左心室功能障碍是化疗后最常见的心脏并发症。对于改善该癌症人群的心脏预后而言,检测和早期治疗是主要问题。心脏毒性最常见的定义是左心室射血分数(LVEF)降低10个百分点,降至<53%。化疗引起的心肌损伤可能是一个连续过程,始于心脏生物标志物升高,随后出现结构性心肌变形,导致LVEF下降。在开始化疗前,必须确定个体化风险特征(取决于年龄、心血管危险因素、化疗类型、基线肌钙蛋白、基线整体纵向应变和基线LVEF),以考虑心脏保护治疗。迄今为止,尚无证据表明所有癌症患者都需要进行系统性心脏保护治疗(血管紧张素转换酶抑制剂和/或β受体阻滞剂)。然而,对于亚临床左心室功能障碍患者,早期心脏保护治疗在预防心脏事件方面似乎很有前景。