Department of Tropical Hygiene, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand.
Mahidol-Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand.
Malar J. 2019 Mar 8;18(1):64. doi: 10.1186/s12936-019-2704-3.
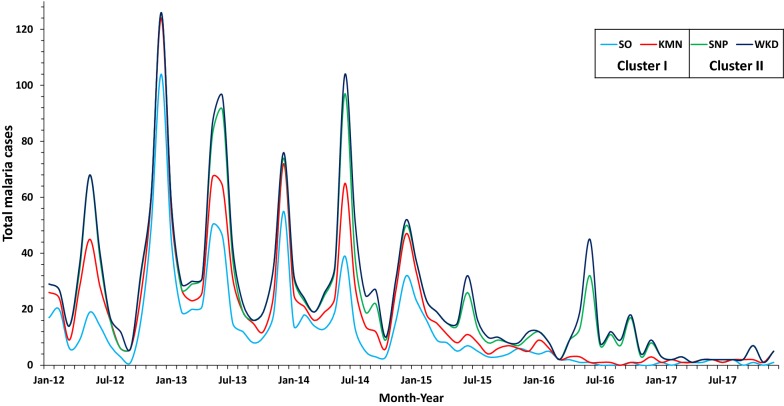
Malaria is heterogeneously distributed across landscapes. Human population movement (HPM) could link sub-regions with varying levels of transmission, leading to the persistence of disease even in very low transmission settings. Malaria along the Thai-Myanmar border has been decreasing, but remains heterogeneous. This study aimed to measure HPM, associated predictors of travel, and HPM correlates of self-reported malaria among people living within malaria hotspots.
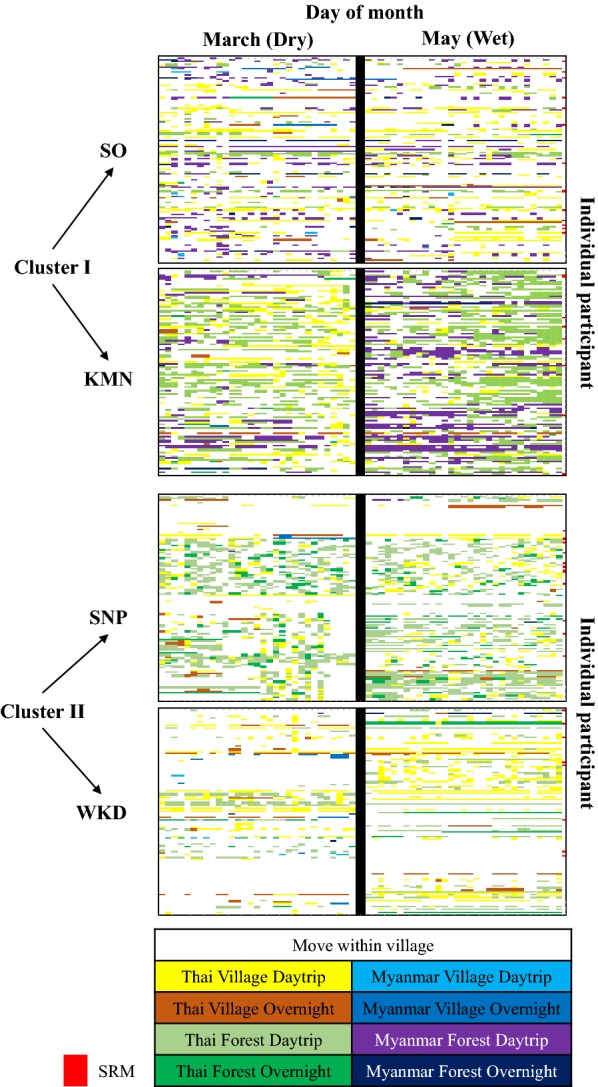
526 individuals from 279 households in two malaria hotspot areas were included in a prospective observational study. A baseline cross-sectional study was conducted at the beginning, recording both individual- and household-level characteristics. Individual movement and travel patterns were repeatedly observed over one dry season month (March) and one wet season month (May). Descriptive statistics, random effects logistic regressions, and logistic regressions were used to describe and determine associations between HPM patterns, individual-, household-factors, and self-reported malaria.
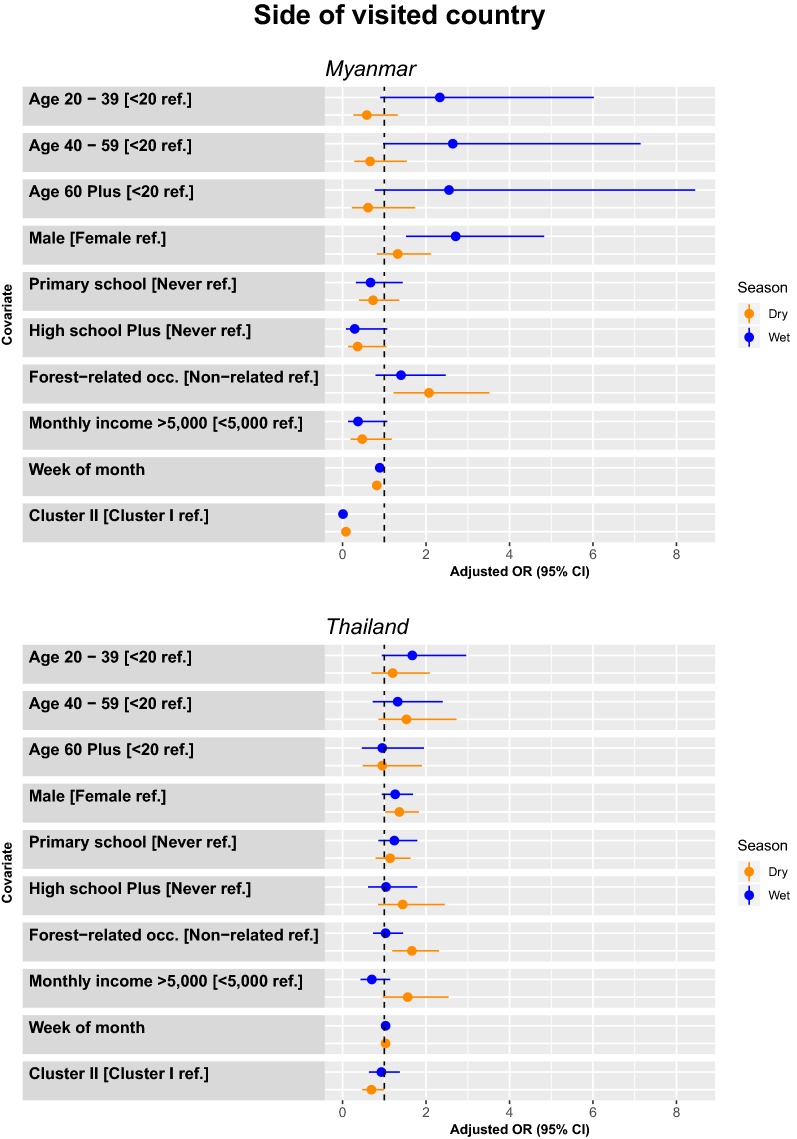
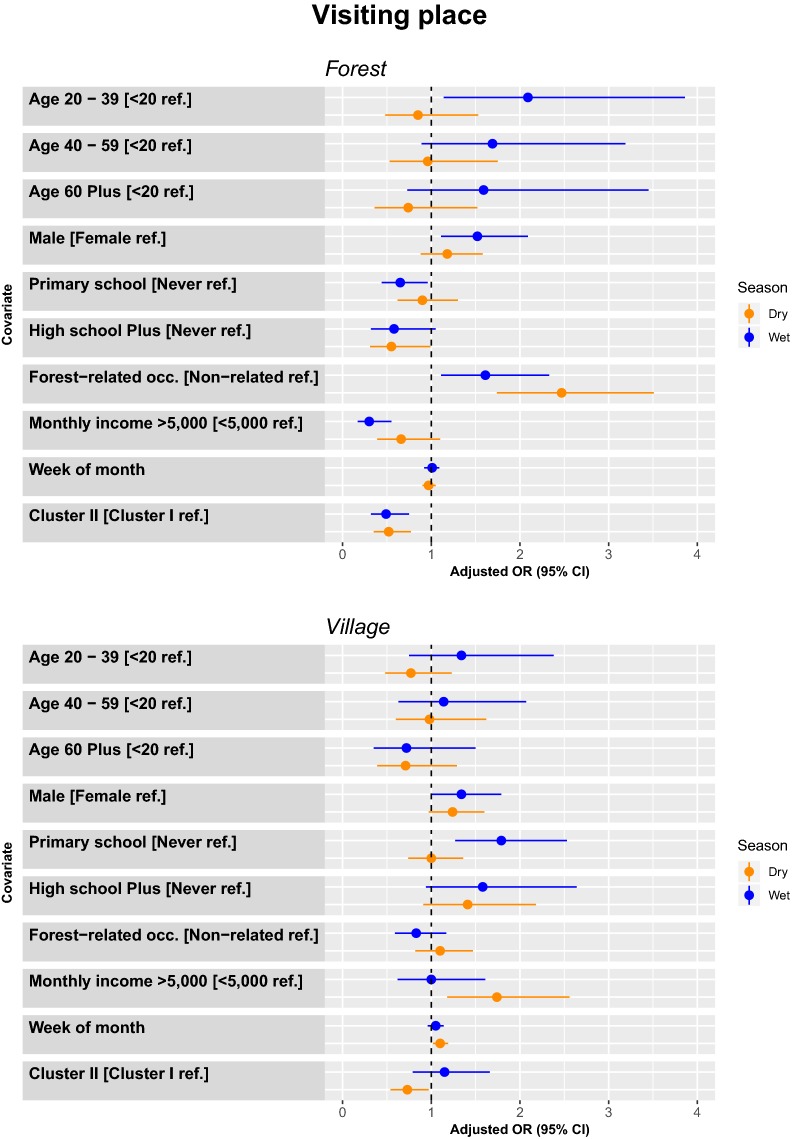
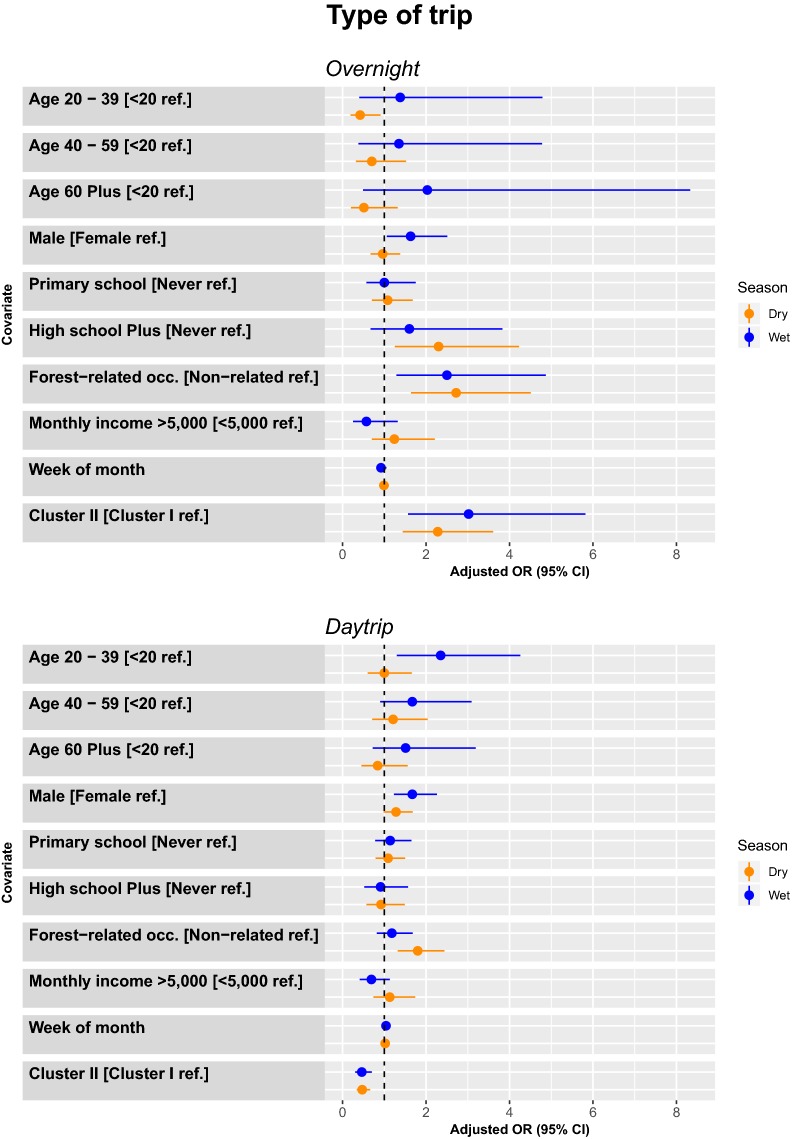
Trips were more common in the dry season. Malaria risk was related to the number of days doing outdoor activities in the dry season, especially trips to Myanmar, to forest areas, and overnight trips. Trips to visit forest areas were more common among participants aged 20-39, males, individuals with low income, low education, and especially among individuals with forest-related occupations. Overnight trips were more common among males, and individual with forest-related occupations. Forty-five participants reported having confirmed malaria infection within the last year. The main place of malaria blood examination and treatment was malaria post and malaria clinic, with participants usually waiting for 2-3 days from onset fever to seeking diagnosis. Individuals using bed nets, living in houses with elevated floors, and houses that received indoor residual spraying in the last year were less likely to report malaria infection.
An understanding of HPM and concurrent malaria dynamics is important for consideration of targeted public health interventions. Furthermore, diagnosis and treatment centres must be capable of quickly diagnosing and treating infections regardless of HPM. Coverage of diagnosis and treatment centres should be broad, maintained in areas bordering malaria hotspots, and available to all febrile individuals.
疟疾在景观中呈异质分布。人类人口流动(HPM)可以将具有不同传播水平的亚区域联系起来,导致疾病即使在传播水平非常低的情况下也能持续存在。泰国-缅甸边境的疟疾一直在减少,但仍然存在异质性。本研究旨在衡量 HPM、与旅行相关的预测因素以及 HPM 与居住在疟疾热点地区的人群中自我报告疟疾之间的相关性。
279 户家庭中的 526 人参加了一项前瞻性观察研究。在旱季(3 月)和雨季(5 月)的一个月内,对两个疟疾热点地区的个人和家庭特征进行了基线横断面研究。反复观察个体和家庭的流动和旅行模式。使用描述性统计、随机效应逻辑回归和逻辑回归来描述和确定 HPM 模式、个体、家庭因素与自我报告疟疾之间的关联。
在旱季,旅行更为常见。疟疾风险与旱季户外活动天数有关,特别是前往缅甸、森林地区和过夜旅行。20-39 岁的参与者、男性、收入低、教育程度低的个体以及从事与森林相关职业的个体更常前往森林地区旅行。过夜旅行在男性和从事与森林相关职业的个体中更为常见。45 名参与者报告在过去一年中确诊患有疟疾感染。疟疾血液检查和治疗的主要场所是疟疾哨所和疟疾诊所,参与者通常在发热后等待 2-3 天才能进行诊断。过去一年中使用蚊帐、居住在架空地板房屋和接受室内残留喷洒的个体不太可能报告疟疾感染。
了解 HPM 和并发疟疾动态对于考虑有针对性的公共卫生干预措施很重要。此外,诊断和治疗中心必须能够快速诊断和治疗感染,无论 HPM 如何。诊断和治疗中心的覆盖范围应该广泛,维持在疟疾热点地区的边界,并且对所有发热患者开放。