Centre for Cancer Research and Cell Biology, Queen's University Belfast, Belfast, UK.
Almac Diagnostics Ltd, Craigavon, UK.
Gut. 2019 Nov;68(11):1918-1927. doi: 10.1136/gutjnl-2018-317624. Epub 2019 Mar 9.
Current strategies to guide selection of neoadjuvant therapy in oesophageal adenocarcinoma (OAC) are inadequate. We assessed the ability of a DNA damage immune response (DDIR) assay to predict response following neoadjuvant chemotherapy in OAC.
Transcriptional profiling of 273 formalin-fixed paraffin-embedded prechemotherapy endoscopic OAC biopsies was performed. All patients were treated with platinum-based neoadjuvant chemotherapy and resection between 2003 and 2014 at four centres in the Oesophageal Cancer Clinical and Molecular Stratification consortium. CD8 and programmed death ligand 1 (PD-L1) immunohistochemical staining was assessed in matched resection specimens from 126 cases. Kaplan-Meier and Cox proportional hazards regression analysis were applied according to DDIR status for recurrence-free survival (RFS) and overall survival (OS).
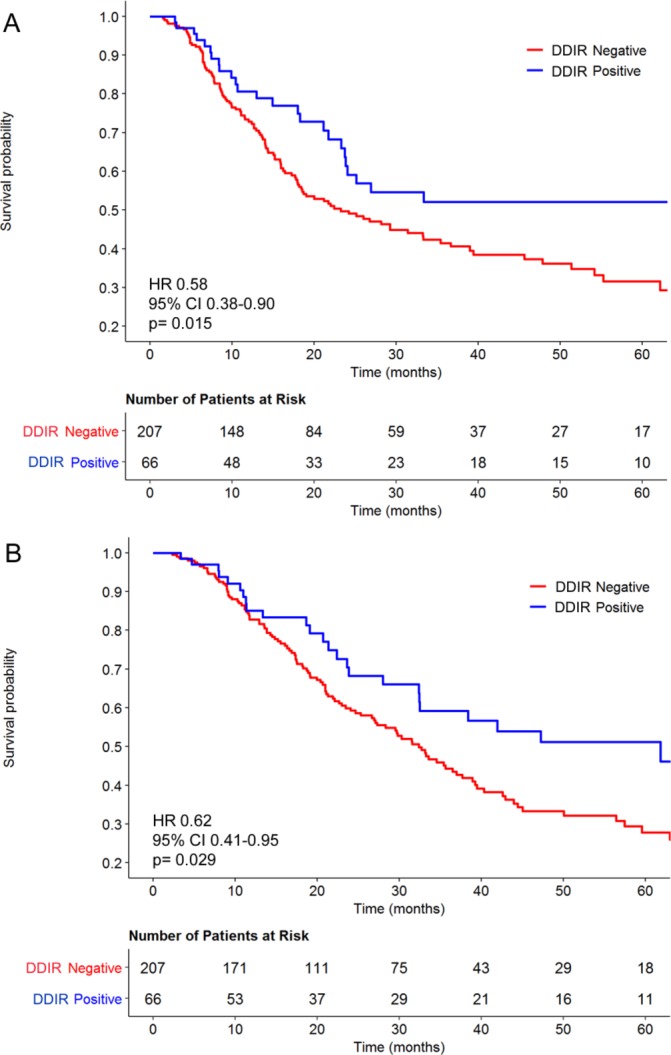
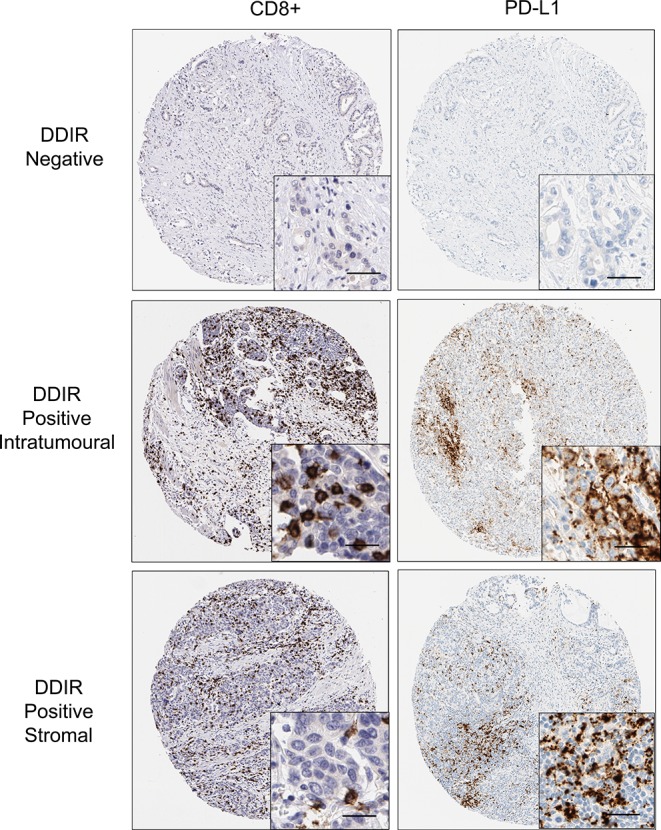
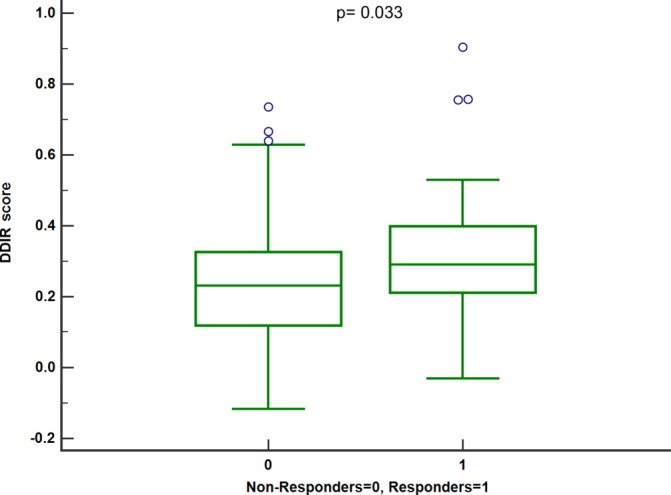
A total of 66 OAC samples (24%) were DDIR positive with the remaining 207 samples (76%) being DDIR negative. DDIR assay positivity was associated with improved RFS (HR: 0.61; 95% CI 0.38 to 0.98; p=0.042) and OS (HR: 0.52; 95% CI 0.31 to 0.88; p=0.015) following multivariate analysis. DDIR-positive patients had a higher pathological response rate (p=0.033), lower nodal burden (p=0.026) and reduced circumferential margin involvement (p=0.007). No difference in OS was observed according to DDIR status in an independent surgery-alone dataset.DDIR-positive OAC tumours were also associated with the presence of CD8+ lymphocytes (intratumoural: p<0.001; stromal: p=0.026) as well as PD-L1 expression (intratumoural: p=0.047; stromal: p=0.025).
The DDIR assay is strongly predictive of benefit from DNA-damaging neoadjuvant chemotherapy followed by surgical resection and is associated with a proinflammatory microenvironment in OAC.
目前指导食管腺癌(OAC)新辅助治疗选择的策略还不够完善。我们评估了 DNA 损伤免疫反应(DDIR)检测在预测 OAC 新辅助化疗后反应中的作用。
对 273 例经福尔马林固定石蜡包埋的新辅助化疗前内镜 OAC 活检进行了转录谱分析。所有患者于 2003 年至 2014 年在 Oesophageal Cancer Clinical and Molecular Stratification 联盟的四个中心接受铂类为基础的新辅助化疗和切除术治疗。对 126 例手术标本进行 CD8 和程序性死亡配体 1(PD-L1)免疫组化染色评估。根据 DDIR 状态,对无复发生存率(RFS)和总生存率(OS)进行 Kaplan-Meier 和 Cox 比例风险回归分析。
共有 66 例 OAC 样本(24%)为 DDIR 阳性,其余 207 例样本(76%)为 DDIR 阴性。DDIR 检测阳性与 RFS(HR:0.61;95%CI 0.38 至 0.98;p=0.042)和 OS(HR:0.52;95%CI 0.31 至 0.88;p=0.015)的多变量分析改善相关。DDIR 阳性患者的病理缓解率更高(p=0.033),淋巴结负担更低(p=0.026),环周切缘受累减少(p=0.007)。在独立的手术组数据中,根据 DDIR 状态,OS 无差异。DDIR 阳性的 OAC 肿瘤也与 CD8+淋巴细胞的存在相关(肿瘤内:p<0.001;基质:p=0.026)以及 PD-L1 表达相关(肿瘤内:p=0.047;基质:p=0.025)。
DDIR 检测对接受 DNA 损伤性新辅助化疗联合手术切除的获益具有很强的预测作用,并与 OAC 中的促炎微环境相关。