From the Department of Public Health (E.V., H.F.L., V.C.), Erasmus MC University Medical Center, Rotterdam.
Department of Neurology (E.V., V.C., M.J.H.L.M., D.W.J.D., B.R.), Erasmus MC University Medical Center, Rotterdam.
Stroke. 2019 Apr;50(4):923-930. doi: 10.1161/STROKEAHA.118.024091.
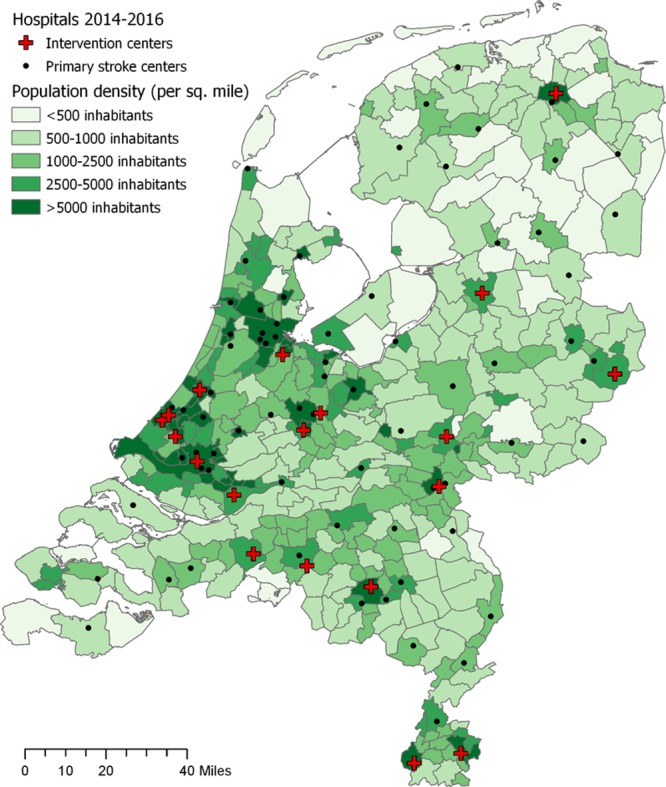
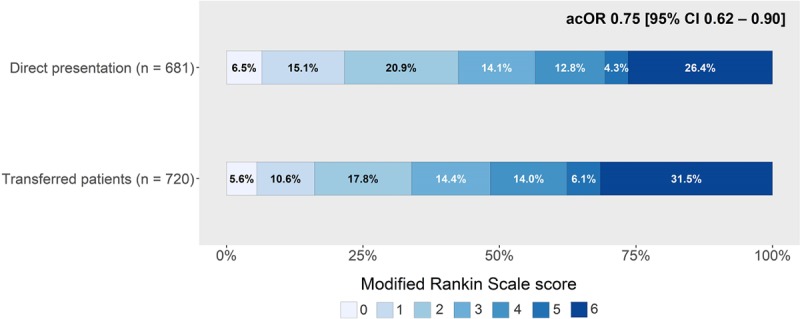
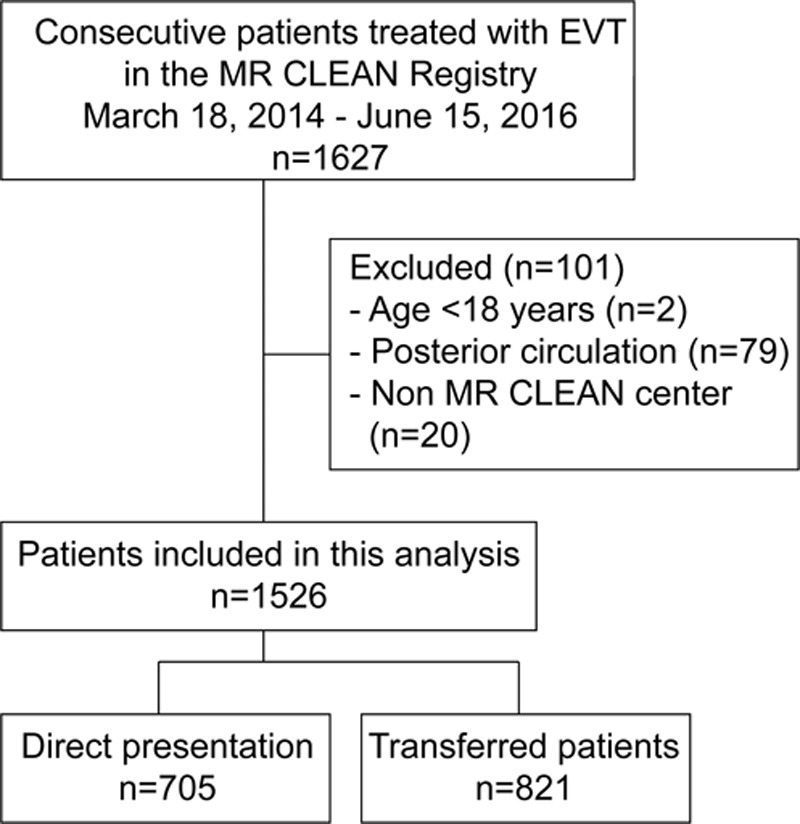
Background and Purpose- To assess the effect of inter-hospital transfer on time to treatment and functional outcome after endovascular treatment (EVT) for acute ischemic stroke, we compared patients transferred from a primary stroke center to patients directly admitted to an intervention center in a large nationwide registry. Methods- MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) Registry is an ongoing, prospective, observational study in all centers that perform EVT in the Netherlands. We included adult patients with an acute anterior circulation stroke who received EVT between March 2014 to June 2016. Primary outcome was time from arrival at the first hospital to arterial groin puncture. Secondary outcomes included the 90-day modified Rankin Scale score and functional independence (modified Rankin Scale score of 0-2). Results- In total 821/1526 patients, (54%) were transferred from a primary stroke center. Transferred patients less often had prestroke disability (227/800 [28%] versus 255/699 [36%]; P=0.02) and more often received intravenous thrombolytics (659/819 [81%] versus 511/704 [73%]; P<0.01). Time from first presentation to groin puncture was longer for transferred patients (164 versus 104 minutes; P<0.01, adjusted delay 57 minutes [95% CI, 51-62]). Transferred patients had worse functional outcome (adjusted common OR, 0.75 [95% CI, 0.62-0.90]) and less often achieved functional independence (244/720 [34%] versus 289/681 [42%], absolute risk difference -8.5% [95% CI, -8.7 to -8.3]). Conclusions- Interhospital transfer of patients with acute ischemic stroke is associated with delay of EVT and worse outcomes in routine clinical practice, even in a country where between-center distances are short. Direct transportation of patients potentially eligible for EVT to an intervention center may improve functional outcome.
背景与目的-为了评估在急性缺血性卒中血管内治疗(EVT)后,医院间转运会对治疗时间和功能结局的影响,我们比较了从初级卒中中心转来的患者和直接收入介入中心的患者在一个大型全国登记处的情况。方法-MR CLEAN(荷兰急性缺血性卒中血管内治疗多中心随机临床试验)登记处是荷兰所有行 EVT 中心的一项正在进行的前瞻性观察性研究。我们纳入了急性前循环卒中且于 2014 年 3 月至 2016 年 6 月期间接受 EVT 的成年患者。主要结局是从到达第一家医院到动脉腹股沟穿刺的时间。次要结局包括 90 天改良 Rankin 量表评分和功能独立性(改良 Rankin 量表评分 0-2)。结果-在总共 1526 例患者中,821 例(54%)是从初级卒中中心转来的。转院患者既往卒中残疾的比例较低(227/800[28%]与 255/699[36%];P=0.02),更常接受静脉溶栓(659/819[81%]与 511/704[73%];P<0.01)。与直接收入介入中心的患者相比,转院患者从首诊到腹股沟穿刺的时间更长(164 分钟比 104 分钟;P<0.01,调整后延迟 57 分钟[95%CI,51-62])。转院患者的功能结局较差(调整后常见比值比,0.75[95%CI,0.62-0.90]),功能独立性的比例较低(244/720[34%]与 289/681[42%],绝对风险差异-8.5%[95%CI,-8.7 至-8.3])。结论-在常规临床实践中,急性缺血性卒中患者的医院间转运会导致 EVT 延迟和结局较差,即使在中心间距离较短的国家也是如此。将有条件行 EVT 的患者直接转运到介入中心可能会改善功能结局。